|
|
Home | Switchboard | Unix Administration | Red Hat | TCP/IP Networks | Neoliberalism | Toxic Managers |
| (slightly skeptical) Educational society promoting "Back to basics" movement against IT overcomplexity and bastardization of classic Unix | |||||||
| Home | 2020 | 2019 | 2018 | 2017 | 2016 | 2015 | 2014 | 2013 | 2012 | 2011 | 2010 | 2009 |
For the list of top articles see Recommended Links section
|
|
Switchboard | ||||
| Latest | |||||
| Past week | |||||
| Past month | |||||
apa.org
Stress is often described as a feeling of being overwhelmed, worried or run-down. Stress can affect people of all ages, genders and circumstances and can lead to both physical and psychological health issues. By definition, stress is any uncomfortable "emotional experience accompanied by predictable biochemical, physiological and behavioral changes." 1 Some stress can be beneficial at times, producing a boost that provides the drive and energy to help people get through situations like exams or work deadlines. However, an extreme amount of stress can have health consequences and adversely affect the immune, cardiovascular, neuroendocrine and central nervous systems. 2
How stress harms your health
In addition, an extreme amount of stress can take a severe emotional toll. While people can overcome minor episodes of stress by tapping into their body's natural defenses to adapt to changing situations, excessive chronic stress, which is constant and persists over an extended period of time, can be psychologically and physically debilitating. Unlike everyday stressors, which can be managed with healthy stress management behaviors, untreated chronic stress can result in serious health conditions including anxiety, insomnia, muscle pain, high blood pressure and a weakened immune system. 3 Research shows that stress can contribute to the development of major illnesses, such as heart disease, depression and obesity. 4
Some studies have even suggested t hat unhealthy chronic stess management, such as overating "comfort" foods, has contributed to the growing obesity epidemic. 5
Yet, despite its connection to illness, APA's Stress in America survey revealed that 33 percent of Americans never discuss ways to manage stress with their healthcare provider.
Chronic stress can occur in response to everday stressors that are ignored or poorly managed, as well as to exposure to traumatic events. The consequences of chronic stress are serious, particularly as it contributes to anxiety and depression. People who suffer from depression and anxiety are at twice the risk for heart disease than people without these conditions. 6 Additionally, research has shown that there is an association between both acute and chronic stress and a person's abuse of addictive substances. 7
Managing your stress
Studies have also illustrated the strong link between insomnia and chronic stress. 8
According to APA's Stress in America survey, more than 40 percent of all adults say they lie awake at night because of stress. Experts recommend going to bed at a regular time each night, striving for at least seven to eight hours of sleep and eliminating distractions such as television and computers from the bedroom. Many Americans who experience prolonged stress are not making the lifestyle changes necessary to reduce stress and ultimately prevent health problems.
Improving lifestyle and behavioral choices are essential steps toward increasing overall health and avoiding chronic stress. The key to managing stress is recognizing and changing the behaviors that cause it, but changing your behavior can be challenging. Taking one small step to reduce your stress and improve your emotional health, such as going on a daily walk, can have a beneficial effect. Being active is a small but powerful change you can make to manage stress.
Physical activity increases your body's production of feel-good endorphins, a type of neurotransmitter in the brain, and helps in treating mild forms of depression and anxiety. 9 In addition, eating a healthy diet and enhancing both the amount and quality of your sleep may be beneficial. But remember, if a high stress level continues for a long period of time, or if potential problems from stress continue to interfere with activities of daily living, it is important to reach out to a licensed mental health professional, such as a psychologist. Research has shown that chronic stress can be treated with appropriate interventions such as lifestyle and behavior change, therapy, and in some situations, medication. 10
A psychologist can help you ovecome the barriers that are stopping you from living a healthy life, manage stress effectively and help identify behaviors and situations that are contributing to your consistently high stress level.
Special thanks to Mary K. Alvord, PhD, Karina W. Davidson, PhD, Jennifer F. Kelly, PhD, ABPP, Kevin M. McGuiness, PhD, MS, ABPP-CH, and Steven Tovian, PhD, ABPP, who assisted with this article.
ReferencesThe full text of articles from APA Help Center may be reproduced and distributed for noncommercial purposes with credit given to the American Psychological Association. Any electronic reproductions must link to the original article on the APA Help Center. Any exceptions to this, including excerpting, paraphrasing or reproduction in a commercial work, must be presented in writing to the APA. Images from the APA Help Center may not be reproduced.
- Baum, A. (1990). "Stress, Intrusive Imagery, and Chronic Distress," Health Psychology , Vol. 6, pp. 653-675.
- Anderson, N.B. (1998). "Levels of Analysis in Health Science: A Framework for Integrating Sociobehavioral and Biomedical Research," Annals of the New York Academy of Sciences , Vol. 840, pp. 563-576.
- Baum, A. & Polsusnzy, D. (1999). "Health Psychology: Mapping Biobehavioral Contributions to Health and Illness." Annual Review of Psychology , Vol. 50, pp. 137-163.
- Ibid.
- Dallman, M. et al. (2003). "Chronic stress and obesity: A new view of 'comfort food.'" PNAS, Vol. 100, pp. 11696-11701.
- Anderson, N.B. & Anderson, P.E. (2003). Emotional Longevity: what really determines how long you live. New York: Viking.
- Sinha, R. (2008). "Chronic Stress, Drug Use, and Vulnerability to Addiction." Annals of the New York Academy of Sciences , Vol. 1141, pp. 105-130.
- Vgontzas, A.N. et al. (1997). "Chronic insomnia and activity of the stress system: a preliminary study." Journal of Psychosomatic Research , Vol. 45, pp. 21-31.
- Fox, K.R. (1999). "The influence of physical activity on mental well-being." Public Health Nutrition , Vol. 2, pp. 411-418.
- McEwen, B.S. (2004). "Protection and Damage from Acute and Chronic Stress: Allostasis and Allostatic Overload and Relevance to the Pathophysiology of Psychiatric Disorders." Annals of the New York Academy of Sciences , Vol. 1032, pp. 1-7.
Dec 12, 2017 | www.nakedcapitalism.com
...Neoliberal epidemics are particular pathways of embodiment. From Ted Schrecker and Clare Bambra in The Conversation :
In our new book , we draw on an extensive body of scientific literature to assess the health effects of three decades of neoliberal policies. Focusing on the social determinants of health -- the conditions of life and work that make it relatively easy for some people to lead long and healthy lives, while it is all but impossible for others -- we show that there are four interconnected neoliberal epidemics: austerity, obesity, stress, and inequality. They are neoliberal because they are associated with or worsened by neoliberal policies. They are epidemics because they are observable on such an international scale and have been transmitted so quickly across time and space that if they were biological contagions they would be seen as of epidemic proportions.
(The Case-Deaton study provides an obvious fifth: Deaths of despair. There are doubtless others.) Case in point for one of the unluckier members of the 90%:
On the morning of 25 August 2014 a young New Jersey woman, Maria Fernandes, died from inhaling gasoline fumes as she slept in her 13-year-old car. She often slept in the car while shuttling between her three, low-wage jobs in food service; she kept a can of gasoline in the car because she often slept with the engine running, and was worried about running out of gasoline. Apparently, the can accidentally tipped over and the vapours from spilled gasoline cost her life. Ms Fernandes was one of the more obvious casualties of the zero-hours culture of stress and insecurity that pervades the contemporary labour market under neoliberalism.
And Schrecker and Bambra conclude:
Neoliberalism operates through labor markets to undermine health not only by way of the financial consequences of unemployment, inadequate employment, or low wages, as important as these are, but also through chronic exposure to stress that 'gets under your skin' by way of multiple mechanisms. Quite simply, the effects of chronic insecurity wear people out over the life course in biologically measurable ways .
... ... ...
Oh, and "beyond class" because for social beings embodiment involves "social production; social consumption; and social reproduction." In the most reductive definition of class -- the one I used in my crude 1% + 10% + 90% formulation -- class is determined by wage work (or not), hence is a part of production (of capital), not social consumption (eating, etc.) or social reproduction (children, families, household work ). So, even if class in our political economy is the driver, it's not everything.
nonclassical , December 11, 2017 at 8:30 pm
Amfortas the Hippie , December 11, 2017 at 4:20 pmL.S. reminiscent of Ernst Becker's, "The Structure of Evil" – "Escape from Evil"? (..not to indicate good vs. evil dichotomy) A great amount of perspective must be agreed upon to achieve "change" intoned. Divide and conquer are complicit, as noted .otherwise (and as indicated by U.S. economic history) change arrives only when all have lost all and can therefore agree begin again.
There is however, Naomi Klein perspective, "Shock Doctrine", whereby influence contributes to destabilization, plan in hand leading to agenda driven ("neoliberal"=market fundamentalism) outcome, not at all spontaneous in nature:
"Neoliberalism sees competition as the defining characteristic of human relations. It redefines citizens as consumers, whose democratic choices are best exercised by buying and selling, a process that rewards merit and punishes inefficiency. It maintains that "the market" delivers benefits that could never be achieved by planning.
Attempts to limit competition are treated as inimical to liberty. Tax and regulation should be minimised, public services should be privatised. The organisation of labour and collective bargaining by trade unions are portrayed as market distortions that impede the formation of a natural hierarchy of winners and losers. Inequality is recast as virtuous: a reward for utility and a generator of wealth, which trickles down to enrich everyone. Efforts to create a more equal society are both counterproductive and morally corrosive. The market ensures that everyone gets what they deserve."
Rosario , December 11, 2017 at 10:55 pmWell done, as usual.
On Case-Deason: Sounds like home. I keep the scanner on(local news) ems and fire only since 2006(sheriff got a homeland security grant). The incidence of suicide, overdose and "intoxication psychosis" are markedly increased in the last 10+ years out here in the wilderness(5K folks in whole county, last I looked). Our local economy went into near depression after the late 90's farm bill killed the peanut program then 911 meant no hunting season that year(and it's been noticeably less busy ever since) then drought and the real estate crash(we had 30 some realtors at peak..old family land being sold off, mostly). So the local Bourgeoisie have had less money to spend, which "trickles down" onto the rest of us.:less construction, less eating out even at the cheap places, less buying of gas, and on and on means fewer employees are needed, thus fewer jobs. To boot, there is a habit among many employers out here of not paying attention to labor laws(it is Texas ) the last minwage rise took 2 years to filter out here, and one must scrutinize one's pay stub to ensure that the boss isn't getting squirrelly with overtime and witholding.
Geography plays into all this, too 100 miles to any largish city.... ... ...
Lambert Strether Post author , December 11, 2017 at 11:20 pmI'm not well versed in Foucault or Lacan but I've read some of both and in reading between the lines of their writing (the phantom philosophy?) I saw a very different message than that often delivered by post-modern theorists.
As opposed to being champions of "self-actualization/identity" and "absolute relativism", I always got the impression that they were both offering stark warnings about diving too deeply into the self, vis-a-vis, identity. As if, they both understood the terrifying world that it could/would create, devoid of common cause, community, and ultimately empathy. A world where "we" are not possible because we have all become "I".
Considering what both their philosophies claimed, if identity is a lie, and the subject is always generated relative to the other, then how the hell can there be any security or well being in self-actualization? It is like trying to hit a target that does not exist.
All potentially oppressive cultural categorizations are examples of this (black, latino, gay, trans, etc.). If the identity is a moving target, both to the oppressor and the oppressed, then how can it ever be a singular source of political action? You can't hit what isn't there. This is not to say that these groups (in whatever determined category) are not oppressed, just that formulating political action based strictly on the identity (often as an essential category) is impossible because it does not actually exist materially. It is an amalgamation of subjects who's subjectivity is always relative to some other whether ally or oppressor. Only the manifestations of oppression on bodies (as brought up in Lambert's post) can be utilized as metrics for political action.
... ... ...
oaf , December 12, 2017 at 7:11 amI thought of a couple of other advantages of the "embodiment" paradigm:
Better Framing . Wonks like Yglesias love to mock working class concerns as "economic anxiety," which is at once belittling (it's all about f-e-e-e-lings *) and disempowering (solutions are individual, like therapy or drugs). Embodiment by contrast insists that neoliberalism (the neoliberal labor market (class warfare)) has real, material, physiological effects that can be measured and tracked, as with any epidemic.
... ... ...
"we have measurable health outcomes from political choices" So True!!!
Thank you for posting this.
Dec 13, 2017 | www.bbc.com
It is hardly surprising then, that we tend to assume that white teeth are not only attractive, but healthy. The hue of our teeth depends on their intrinsic color, influenced in part by our genes and our age, combined with stains from smoking, eating, drinking and taking certain medications. As you get older your teeth often become yellower as the enamel begins to wear away, exposing the dentine beneath .
Green fur
Stains then overlay the yellowing teeth, with foods such as tomato-based sauces and coffee leaving behind colored compounds called chromogens, while bacteria or fungi can cause green, greyish, furry looking stains .
Many of the experiments on tooth colour have been conducted in laboratory test tubes, rather than in the mouths of living people. Often cows' teeth are used because they give researchers with a larger surface area to study, but sometimes extracted human teeth are tested too.
Surprisingly, black tea doesn't stain the teeth unless preceded by white wine
One study conducted by Mark Wolff from New York University soaked cows' teeth for an hour in black tea, red wine or white wine in various configurations. It was no surprise that the red wine left the strongest stains. Surprisingly, the black tea didn't stain the teeth unless it had been preceded by white wine . It seems the acid content of the wine was making the enamel slightly more porous, allowing the tea to leave its mark.
View image of An empty coffee mug stained with coffee (Credit: Alamy)These food and drink-based stains may discolor teeth, but they don't indicate that the teeth are unhealthy. You can have pearly white teeth and still have gum infections or cavities. Likewise, you can have perfectly healthy teeth which are off-white, yellowish or even brownish.
Black stain
There is even one type of stain that some researchers believe might protect against tooth decay. This is the dark edge you sometimes see along teeth at the margins of the gum line. It can look like a series of dark dots. It's known as "black stain".
While the cause of black stain has debated for more than a century, the latest thinking is that it's a special kind of dental plaque comprising calcium, phosphate, various bacteria and some form of iron or copper compound , which gives rise to the black colour.
Curiously, some studies – although not all – have found that children with black stain are less likely to have tooth decay . It's thought that microbes in the stain might be somehow protective.
Just as white teeth aren't necessarily healthy, off-colour teeth aren't necessarily bad either
Of course, in some cases discolouration can indicate decay or other disease, so it is worth getting stains checked out by a dentist. But just as white teeth aren't necessarily healthy, off-colour teeth aren't necessarily bad either.
Mar 23, 2017 | www.nakedcapitalism.com
djrichard, March 22, 2017 at 5:35 pmhuman , March 22, 2017 at 7:46 pmJust a bit of a thought experiment, building on some thinking from a comment yesterday by jefemt
Paradoxically, we appear to be seeing a coalescence and consolidation of insurers, we will end up being delightfully exceptional, again -- effectively being single-payer, private sector, paying a monopoly an add-on cost of 35-40% to a parasitic industry whose executives and employees do not contribute to the CARE equation.
Taking jefemt's thinking further, imagine the health insurance provider was not only monopolistic (owned the entire market), but was also a GSE (government sponsored enterprise). Now take it one more step and imagine it was an actual part of the government and not merely a GSE.
Conceivably, it wouldn't even have to live off appropriations from congress, assuming it was equally as extractive from the private sector as it is now (i.e. revenue model is the same). Talk about good living. Who knows, maybe they pocket their proceeds into some kind of surplus in Treasury dept.
But let's assume they had to give up on revenue models. [Afterall, it's easier to find partners in congress when you have an appropriations process that binds you to them.] Then they would be exposed. Somebody would get the bright idea that this agency doesn't need as much staffing since they are no longer revenue oriented. That indeed, they could have the same staffing profile as the agency responsible for medicare. Indeed they could be folded into medicare.
I was thinking of this too as a reponse to Why Steve Bannon Wants You to Believe in the Deep State" [Politico]. "Like the Death Star, the American Deep State does not, of course, exist. "
Indeed, I think of the insurance industry as being part of the deep state already. It seems that congress's preference is that this part of the deep state is outsourced. So that's it not a GSE, and not even a monopoly, but maintained as an oligopoly. And then, well hey whatever surplus it can hoover up is fair game. After all free-hand of the market and all that. [And heaven knows, we don't want to crowd that out.]
In contrast to other parts of the deep state that don't really have a revenue model. In which case, those parts need to be insourced by the Fed Gov.
Ernesto Lyon , March 23, 2017 at 12:09 amThe CIA has a long history of drug trafficking. The FBI traffics in blackmail. The NSA in network surveillance. DIA, special ops. NRO, satelite throughput. 11 more in the US of A and countless more globally. They all have opaque resources outside of regular channels.
Great documentary about the 80's cocaine business in Miami called "Cocaine Cowboys." It's real life Scarface. Guess who the Feds sent to get a handle on the cocaine smuggling? See-eye-aye man George H.W. Bush. Coincidence?
Nov 25, 2017 | angrybearblog.com
I have been doing my typical reading on healthcare in the US and ran across several articles which seemingly come together at various points in the dialogue and are written by different authors. I decided to tie them together into a much wider and telling story.
An interesting point being was made by MedPage Today's Dr. Milton Packer on his blog, " people suffer and die because Payors (Healthcare Insurance) is cost effective ." He starts his discussion on the opiate epidemic in the US, opiates are being prescribed by doctors for pain relief and . . .
"Patients are becoming addicted to opiates after the initial 10 day prescription with one-fifth of patients still using opiates a year later. There is no need to prescribe opiates as other less addictive pain-relief formulations are available, which are not commonly prescribed." This raises the question of why?
Payers will not pay for the alternatives. The less-addictive opiates are more expensive and payers have declined to support them. Patients get addicted because prescribing for the lower cost and highly addictive opiates saves the payers money initially (me) .
September 17, 2017, the New York Time and ProPublica (independent, nonprofit investigative journalism organization) collaborated on an article concerning the opiod epidemic in the US.
At a time when the United States is in the grip of an opioid epidemic, many insurers are limiting access to pain medications that carry a lower risk of addiction or dependence, even as they provide comparatively easy access to generic opioid medications.
The reason given: Opioid drugs are generally cheap while safer alternatives are often more expensive.
While the pharmaceutical manufacturers, distributors , and doctors have come under scrutiny; insurance companies and the pharmacy benefit managers (CVS Caremark, Express Scripts and OptumRx) make the final decisions as to what is covered. It could be something as simple as a higher tier and deductible to block usage.
A little side trip here and a continuation of the above. A week or so ago, I ran across another MedPage Today article by Dr. Packer; " Who Actually Is Reviewing All Those Preauthorization Requests and How the System Works ." Dr. Packers was giving a talk on advances in medicine with regard to heart failures to a room of about 20 or so doctors who were retired.
Since many of them were no longer involved in active patient care, he wondered why they might want to hear a presentation on new advances in heart failure. Here was their answer:
Doctors: " We no longer care for patients, but we care about what's going on. You see, most of us are employed by insurance companies to do preauthorization for drugs and medical procedures ."
" Dr. Packer: I just gave a talk about new drugs for heart failure. Are you responsible for preauthorizing their use for individual patients? "
The answer; "Yes."
" So did I say anything today that was helpful? I talked about many new treatments. Did I say anything that you might use to inform your preauthorization responsibilities? "
"Oh, we've heard about those drugs before. We are asked to approve their use for patients all the time; but, we don't approve most of the requests. Nearly all of them are outside of the guidelines we are given."
" I just showed you evidence that these new drugs and devices make a real positive difference in people's lives. People who get them feel better and live longer. "
"Yes, you were very convincing. But the drugs are too expensive. So we typically reject requests, at least the first time. We figure that, if doctors are really serious, then they should be willing to make the request again and again."
" If the drugs will help people, how can you say no? "
"You see, if it weren't for us, the system would go broke. Every time we say yes, healthcare becomes more expensive, and that isn't a good thing. So when we say no, we are keeping the system in balance. Our job is to save our system of healthcare."
" But you are not saving our healthcare system. You are simply making money for the company that you work for. And patients aren't getting the drugs that they need. "
"You really don't understand, do you? If we approve expensive drugs, then the system goes broke. Then no one gets healthcare."
"Plus, if I approve too many expensive drugs, I won't get my bonus at the end of the month. So giving out too many approvals wouldn't be a smart thing for me to do. Would it?"
Now before you start on insurance companies and doctors; understand, this is not as free a market place as many would assume.
In all of their political wisdom, Congress favors pharmaceutical companies over doctors, insurance companies, and the welfare of the constituents.
Through legislation, Congress has made it impossible for insurance companies to negotiate pharmaceutical pricing in Medicare Part D insurance and also the ACA .
Furthermore with the consolidation happening in healthcare, negotiation by insurance companies with a consolidating and growing healthcare industry is becoming more and more difficult as the former does not have as great of leverage. You have read my argument calling out of Single Payor, Medicare-for-All, Public Option, etc. as the cure for today's healthcare issues and rising cost not being enough as the ACA and Part D were specifically blocked or the cost issue unaddressed in the legislation written by Congress. If these issues are not addressed from the very beginning, we will be fighting the same issues with rising costs a decade later with other programs.
At this point, I begin to disagree with Dr. Packers as he goes on to say:
" So we spend more for healthcare than any other country in the world; but, Americans do not get the care they need. There is a simple reason. Treatment decisions are not being driven based on a physician's knowledge or judgment. They are being driven by what payers are willing to pay for. "
It is true that patients may not get some of the healthcare they need at the time due to denial, which can be appealed to the ACA, and can be a tiring process. It could be approved, passed on to patients, resulting in higher premiums the following year, and the Part D Risk Corridor program pay for it if excessive for the present year. What Dr. Packers does not mention is the rising prices and cost of drugs being blamed by pharmaceutical company on R&D, tooling up to manufacture, etc. The counter argument is much of the R&D is funded by the US government through tax deductions and write-offs for pharmaceutical R&D and capital Overhead. Pharmaceutical profits are double digit at ~25% beating out hospital supplies and healthcare insurance, which is already limited in what can be charged back to the insured by the MLR. To blame insurance companies totally for the higher costs in healthcare is false. Furthermore, a doctor's decision do not always lead to less costly cures or practices.
Maggie Mahar of Health Beat Blog would take the subject of costs a step farther and state Medicare will approve anything the FDA approves for usage regardless of the quality of outcome when measured against older proven treatments. Notably the VA does limit its pharmacy and its care is rated higher than that of today's commercial, for-profit healthcare to which most citizens are exposed.
Dr. Donald Berwick, President Obama's proposed appointment for Medicare and who was in charge of Medicare and Medicaid for 17 months stated;
"20 to 30 percent of health spending is 'waste' that yields no benefit to patients, and that some of the needless spending is a result of onerous, archaic regulations enforced by Medicare and Medicaid.
He listed five reasons for what he described as the 'extremely high level of waste.' They are overtreatment of patients, the failure to coordinate care, the administrative complexity of the health care system, burdensome rules and fraud .
Much is done that does not help patients at all and many physicians know it."
That is the same Medicare/Medicaid being touted by many proponents today as an alternative.
Speaking of costs and pricing for pharmaceuticals, there have been recent incidents of skyrocketing costs on particular drugs. A short while ago, I wrote a post concerning the appointment of Alex Araz as the new HHS Secretary replacing Dr. Tom Price. Formerly, Alex Araz was the CEO of the pharmaceutical giant Eli Lilly & Co.'s U.S. division . He also served under George W. Bush administration as the HHS General Counsel and Deputy Secretary. During that stint, he received praise for his management competence with the HHS; although, he did not have a healthcare background prior to this position.
Here it gets interesting when examining what took place during his tenure with Eli Lilly. One of the leading costs identified in pharmaceuticals increases has been in the rising cost of diabetes medication.
"While the Tweeter-in-Chief, Trump tells us presidential campaign contributor Alex Azar will be a 'star' who will lower prescription prices,"
Public Citizen's Peter Maybarduk (Director) had this to say: " Eli Lilly is notorious for spiking prices of a century-old isolated hormone during Azar's tenure as president and vice president. Eli Lilly raised the price of Humalog by 345%, from $2,657.88 per year to $9,172.80 per year.
Maybe President Trump in appointing Alex Azar to be HHS Secretary should have asked the 6 million diabetic Americans whose insulin prices have more than tripled under Azar's watch at Eli Lilly."
This has nothing to do with R&D and has more to do with pharmaceutical companies controlling the market regardless of supply and throughput restricted manufacturing (capacity).
What I have tried to do is tie these articles together into one cohesive story of how the pharmaceutical industry, insurance, and healthcare can have an impact on healthcare costs. For those who are interested, my background does include working in the manufacture of hospital supplies and pharmaceuticals. Using various citations from these articles, I have tried to touch upon the impact of insurance companies, the healthcare industry, government intervention under the HHS, one particular Med in the market place, etc. Overall, what is going on in the marketplace.
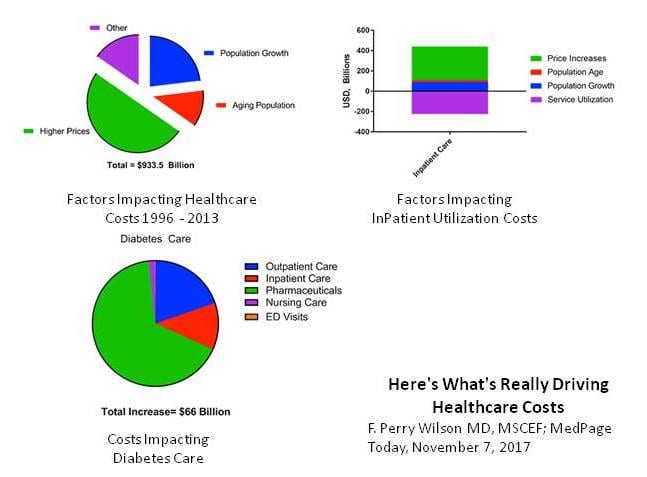
Another article, I read the other day gets into the foundation of what is happening based upon a recently completed study by JAMA. Using this study, the Methods Man, Dr. Perry Wilson (MedPage Today) examines what is driving healthcare costs in his article Here's What's Really Driving Healthcare Costs using data from Factors Associated With Increases in US Health Care Spending, 1996-2013 and the US Disease Expenditure Project . Dr. Wilson breaks it down using three simple charts which I have consolidated to one.
Dr. Perry Wilson starts off making an overall point about the rising cost of healthcare from 1996 to 2013 and stating; "after accounting for inflation, healthcare expenditures increased $933.5 billion from 1996 to 2013."
Going on: "Healthcare expenditures in the US being high and rising rapidly is nothing new, but the study appearing in the Journal of the American Medical Association identifies the exact components of healthcare that are driving those soaring costs. The data from this study suggests traditional economic forces break down in the US healthcare market.
Different chronic diseases have different patterns of price increases. The biggest increase was seen in diabetes care, as you can see here, driven largely by the rising costs of pharmaceuticals."
The Chart breakdowns reveal the various impacts of healthcare costs moving from left to right and then downward:
• 50% of the increase in healthcare costs was simply due to higher prices.
• Inpatient care or Service Utilization (purple) went down from 1996 – 2013 as outpatient treatment increased; however, the price of the remaining inpatient care went up much more – increasing overall inpatient care spending by around $250 billion.
• Different Chronic Diseases have different patterns of price increases. The biggest increase was seen in diabetes care and driven largely by the rising prices of pharmaceuticals.
The takeaway drawn by Dr Perry Wilson: "Regardless of the disease, it is clear, the price of what we're buying – whether a drug, an ED visit, or a hospital stay – not the amount of what we're buying is the major driver of cost increases . Efforts to reduce the consumption of healthcare may not bend the cost curve as much as efforts to reduce its price."
You can not make an argument about the regulation of costs "not" being one of the dynamic components of a healthcare plan given the continuous unhindered industry driven rising cost of healthcare. Yet, every healthcare plan I have read fails to mention cost regulation specifically, provide remedy for it, and many assume a natural occurrence of control.
Tags: run75441 Comments (9) Digg Facebook Twitter Comments (9)
Longtooth , November 26, 2017 12:59 am
Longtooth , November 26, 2017 1:08 amRun thanks for this, but in my opinion you're avoiding the central problem , though you briefly touched upon it without being more explicit:
"This has nothing to do with R&D and has more to do with pharmaceutical companies controlling the market regardless of supply and restricted manufacturing throughput. "
The market can't be controlled by the pharmaceutical companies unless the government lets them. So this is a government sourced and caused problem unless you believe laissez-fair is the gov'ts job to promote and endorse.
You can't blame the pharmaceutical companies for doing precisely what the gov't lets them do by law.. the pharmaceuticals company's owners are in this to be philanthropic are they?
What you are essentially not coming to grips with is that our government is not designed to be democratic but designed by it's concept to be a system to ingratiate those who pay the most to keep the gov't in power which is to say those that represent them are paid to do their bidding in other words a gov't controlled by the sources of wealth to maintain it. if it were anywhere near a democratic system, how could 1% control it?
Longtooth , November 26, 2017 1:36 amRun, sorry I forgot that there's never been a democratic system from the Spartan through the Athenian to the present that hasn't been controlled by the wealth. There have only been moments brought about by extreme deprivation that have had to deal with that deprivation to avoid revolution.
When we want to fix U.S. healthcare costs and quality we know how to do it, but you have to fix the system of government we employ to do it. Address the source of the problem rather than effects of it.
Denis Drew , November 26, 2017 9:29 amRun, let me only add that I don't know how we can have a free market based and biased system of government and anything even approximating a democratic system at the same time. That is the actual dilemma since they are mutually exclusive.
If you think about how to "comprise" one with the other then you have to decide how such compromise is made and sustained (sustained being key word) and I can't see or find any evidence in U.S. history that suggests such compromise has ever worked to provide for the greater good on a sustained basis.
Perhaps its not even possible among human systems of civilized government .. but then why the charade as if it is? If the public wants to improve the healthcare system then why does it elect Presidents and representatives who don't want to improve it? If the public want's to improve the healthcare system why do Supreme Court interpret the Constitutional "law" to prevent it? Or if the 200+ year old constitutional law is so outdated as to be irrelevant than why doesn't the pubic demand to change it?
Or does the pubic want it's cake and eat it too? The public may be confused (I'm sure of this in fact) because they want simultaneously mutually exclusive conditions.
run75441 , November 26, 2017 11:40 amRun, great major post.
Long, " I don't know how we can have a free market based and biased system of government and anything even approximating a democratic system "
No? Look at continental Europe -- look at across the board labor union density -- look at sector-wide labor agreements. Come to think look at our northern neighbor.
Mostly all other problems from health care to student debt to everything are just symptomatic of the same economic/political-union free pathology. Bernie and Eliz don't spend a lot of time looking abroad either -- or even looking at 1973 stateside.
Come a Dem Congress I think the best idea is:
Why Not Hold Union Representation Elections on a Regular Schedule?
Published November 1st, 2017 – Andrew Strom
https://onlabor.org/why-not-hold-union-representation-elections-on-a-regular-schedule/This can be sold as taking a page from Repub govs (e.g., Walker) who force government employee unions to re-certify every year -- with majority of union members, not just those who vote, required to retain.
I'm playing with the idea of proposing (via spam mail*) re-certification for every union in the country every year -- oh, of course, that would include certification elections for every nonunion workplace: that's the Trojan Horse .
We really want to certify/recertify every three or five years (three at first while we are trying to build density -- maybe five later on). Once we organize enough we can write the rules any way we want. By proposing re-certification every year (from my spider hole in Chicago) maybe I can get union members dander up and thereby at least wake them up to the issue. Cab driver political drama.
(* I have about 2000 email addresses, journalists, union, academic, politicians -- in WA, OR, CA, NV -- that I like to hit with new ideas.)
Longtooth , November 26, 2017 5:48 pmDenis:
You may want to look at this again. A portion of it was blocked due to an error in linking to an article on Pharma costs which was kind of important. I have another article coming out which will discuss Pharmaceutical companies pulling advertising from medical news sites and mags if they are critical of pharma. As I read each of these articles, I could see a similar thread in them.
in 2015, AARP broke ties with MetLife over LTC insurance which MetLife discontinued in 2011 (no new applications). No big deal except AARP never told its membership of the AARP sponsored insurance break with MetLife. AARP now has a new LTC insurer New York Life announced as of 2015 and no letter to its members holding MetLife policies. Those who had AARP sponsored MetLife are now left with MetLife who is requesting a 21.75% increase just for cost over 3 years in addition to the normal inflation factor which was ~10% for 2018. AARP refers all inquiries to MetLife even though documents from MetLife still has AARP logos on it. Another interesting post of companies and Organizations screwing people.
JackD , November 26, 2017 9:22 pmDennis,
FWIW I come from a long line of union activists, members, and in one case a major union leader in the western U.S. and California in particular -- Building & Construction Trades Council.
I've been and remain a hugely strong union supporter. However my uncle (the Western US major union leader) was a realist and well understood the nature of economics viz-a-viz unions and capital owners.
In a series of discussions while I resided with he and his wife during one summer college break, he made me understand those trade-offs, and what drove them. At the time the college educated workforce in the US was 10% (4 year or better degree). He said a major factor in union's was the level of the college educated workforce and he said in 1966, that if the rate of college degree growth reached the then unprecedented rate of ~ 0.5%/year than in a few decades 1/3rd of the workforce would have college degrees -- the upshot of which is that they would very unlikely be persuaded to join unions or create new ones. His prognosis in 1966 turns out to be pretty close to reality even though he had little historic information to go on., .. he was not a pie in sky type, but a practical and major proponent of the general working class an working poor.
He also told me in 1966 that if unions demanded too much of the capital owners profits, they would resort to capital invested in automated methods -- his primary example of which was the hift to lath & plaster skilled union members to wall board which required no skill per-se and that forced union wages for interior "plasterers" down as lower skill and more efficient "sheetrock" hangers too over.
He cited other examples of automation replacing skilled union labor and without elaborating it was an eye-opener for me to see that unions were on their way down He not only knew the economics of building and construction business and labor, but of mining and manufacturing.
This was all long before Reagan's anti-unionism push (which in reality was Reagan using what was already well underway as a means of pumping up is conservative credentials).
My uncle's wisest advice was that if unions demanded more than capital owners were able to profit, they would simply use their capital in other enterprises where profits were greater -- this included not only investing in automated methods in mfg'ing and the building and construction trades (remember "sheetrock") , but in foreign low wage labor regions where especially mfg'ed goods could be produced at lower costs IF(the big IF in 1966) transportation and import duties made it more profitable to do so. He cited Mexico as the primary source of low transport cost low wage labor at the time, and at that time import duties from the few mfg'ed goods produced in Mexio were excessive which was the only reason mfg'ing hadn't shifted to use Mexican labor in Mexico for production and also why mfg'ing was investing more and more capital in automation. BUT, he said sooner or later it would become clear that capital owners would push to chane US import policies from Mexican roduced goods and the this would reduce mfg'ing's need for U.S. labor, thus Union's would have far less leverage to take a share of capital profits.
So he was a few decades off in his estimates, but he was right in 1966.. My uncle was among those in the U.S. union leaders who all understood all this very well what they said in public was different that what they saw occurring and would continue to occur they just didn't know then the rate of occurrence -- the computer age hadn't started . semi-conductors were being invented and barely developed for example. China's opening up hadn't occurred yet either. Clinton's NAFTA was still far in the future.
Through al the years since 1966 I've watched the progression of what my Uncle told me during our discussions in the summer of 1966. take place, for precisely the reasons he (and other major union leaders) knew they would.
In hindsight what fails in the U.S. relative to Europe is Germany's constitutional protections of labor unions. which by osmosis transfers to the other major European nations just as U.S. union wages and benefits transferred by the same osmosis to non-union wages and benefits rising to keep pace.
Keep up the good fight, Dennis, but you're forgetting about the economic realities in the US and it's individualism worship and constitution that protects it. .
JimH , November 27, 2017 10:28 amRun, as you know, nothing substantive on controlling medical costs can possibly occur with Republicans in charge. With Democrats in charge, it's tough enough. Witness the ACA's development and the impact of the blue dogs.
Daniel Becker , November 27, 2017 5:22 pmJackD wrote "Run, as you know, nothing substantive on controlling medical costs can possibly occur with Republicans in charge."
I could not agree with you more.
The Republicans' implementation of Medicare Part D which forbids negotiation of drug prices was asinine. Where was their concern for the national deficits and debt?
On heath care President Obama was negotiating with the duplicitous. His opposition had only one concern, their oath to Grover Norquist.
It's not just that pharma has some say on what gets published, but in the health literature world, the trend was to only publish positive results.
As you can imagine, this has left a major void in truly understanding what happens in the body when a treatment is applied. There is a push to change this. Additionally, there is the push toward the idea of "numbers to treat". That is, how many have to receive the treatment to create one positive results. Outcomes can look a lot more different when looking at numbers to treat.
Nov 30, 2017 | marknesop.wordpress.com
Patient Observer , November 27, 2017 at 5:12 pm
Mark, today's posting provided is a nice change of pace to a topic of local impact (for me at least). UGC presented a good overview peppered with supporting data.marknesop , November 28, 2017 at 12:10 amIn an earlier career incarnation, I worked as a systems analyst involved with development of online systems for state social services. Data showed that our systems were able to administer a comprehensive health care program for social services recipients for about 3-4% of the cost of services. Private medical insurance providers required approximately 20% of the cost of services to provide similar services. Yet, private providers were supposedly driven by invisible market forces to maximum efficiency. BS. In fact, they are driven by greed and they found it much easier to maximize profits by colluding with politicians and health care providers. That is the trouble with free markets – its just so damn easy to cheat and cheaters are never in short supply.
One more thing, prescription drugs costs may exceed $600 billion in the US by 2021:
That would be nearly $2,000 per year for every American!
If a tiny fraction of that amount were spent on prevention, education, improved diets and other similar initiatives, the population ought to be healthier and richer. But, greed overpowers the public good every time. The US health care system is a criminal enterprise in my opinion. The good that it does is grossly outweighed by greed and exploitation of human suffering.
I believe the author is also a systems analyst, so you are thinking along similar lines.ucgsblog , November 28, 2017 at 4:05 pmI agree with that. Plus, it seems like they have an entire staff dedicated to giving their "customer" the run around. A friend of mine had to deal with several different departments regarding his healthcare bill. The billing office told him that they only deal with billing questions, and that for explanations for the bill, he should call the doctor's office. The doctor's office told him to call the hospital, since that's where the service took place. The hospital told him to call his primary doctor, who sent him there, and his primary doctor referred him back to the specialist, where he was referred back to the billing department, which promptly told him that they're closing for the day, since he spent 6 hours being transferred from one department to the next.
Nov 30, 2017 | marknesop.wordpress.com
[email protected] , November 27, 2017 at 6:02 pm
I find it terribly silly that we should even consider med student's debt as an excuse. First, American doctors are the best paid professionals in the country. Internists make a median 190 thousand a year, and they are among the worst paid specialties. I cannot possibly see the problem with paying your income for 5 years, knowing that you get access to a caste that will allow you make good money into your eighties.ucgsblog , November 28, 2017 at 4:08 pmSecond, the debt is not that high as you claim. Harvard Medical School tuition is 64 thousand. You can rent across the street with 20 thousand a year – I currently live there.
Third, med students know all this. The reason why they borrow far more is because they know they can afford it. I went to med school somewhere in a developing world. We shared toilets in the dorm. As a matter of fact, most under-30s in Boston live in shared accommodation. The outliers? Med students. Even the lowly Tufts and BU students that I met own cars and live by themselves, mainly in new buildings across the street from their hospitals.
Every time I go to the doctors, I am thinking how I am going to sue their asses if they make a mistake.
It's not an excuse. It's a bill. When you rent an apartment, did you know that most landlords also factor in the property tax when figuring out what your rent payment should be? Similarly, the interest payments on the doctoral students' loans are passed off to the consumer, and that is yet another reason why Healthcare is so expensive. That's why I think that medical school should be free for those students who promise to charge their patients no more than x amount of money.
Nov 30, 2017 | marknesop.wordpress.com
Ryan Ward , November 28, 2017 at 3:40 am
With health care in general, there's a bit of a trade-off. The most cost-efficient systems, like the system in Sweden for example, are fairly regimented and don't leave much room for individual choice (unless someone pays out of pocket for treatment completely outside the public system). On the other hand, systems that give people a little more choice, like the system in Germany, tend to be a little on the pricey side. I think, given American political culture, something along the lines of the German model is much more likely to attract widespread public support. In any case, it's still cheaper than the American system, and achieves some of the best results in the world. https://en.wikipedia.org/wiki/Healthcare_in_Germany
Nov 30, 2017 | marknesop.wordpress.com
James lake , November 28, 2017 at 12:21 am
This is s very interesting insight into healcare in the USA. The cost is shocking.marknesop , November 28, 2017 at 10:25 am
I live in the UK and the healthcare system is paid for from taxation.
When it was established over 70 years ago it's
The health service would be available to all and financed entirely from taxation, which meant that people paid into it according to their means.
It was the best thing in my view that government has ever done.
Good healthcare should be available to all and not dependent on peoples ability to pay.However there always a private healthcare system that ran alongside it
And over the years it had been unpicked as successive governments have tried to privatise it. Claiming they will save the taxpayer money
– opticians and dentistry have become part private after 18 if you are employed.
Which many people do not mind.
-Elderly care was also privatised as it's the most expensive
-care for the disabled also is a issue for local councils
-Mental health became care in the community – society's problem!Privatisation has meant profits for businesses, poor services to vulnerable groups.
And yet still more and more taxation is needed for the NHS!
The issue of more money was even part of the Brexit debate as it was stated that leaving the EU would mean more money for the NHS which people are proud of.There was a quote I was thinking of using in the lead-in, but decided in the end not to since I didn't want to have too many and it might have become confusing. It related that you would get the best medical care of your lifetime – after you died, when they were rushing to save your organs, for transplant. Obviously this would not be true if you were not an organ donor (at least in this country) or died as the result of general wasting away so that you had nothing left which would be particularly coveted. But this is a major issue in medicine in some countries and there have been various lurid tales of bodies being robbed of their organs without family permission, bodies of Ukrainian soldiers harvested of their organs and rackets in third-world countries where the poor or helpless are robbed of organs while they are alive. From my standpoint, since I haven't done much research on it, I have seen little proof of any of them despite plenty of allegation, but it is easy to understand that traffic in organs to those who will pay anything to live a little longer would be tremendously profitable, and the potential for disproportionate profit seldom fails to draw the unscrupulous.Patient Observer , November 28, 2017 at 12:49 pmAs I alluded in the lead-in, Canada has what is sometimes described as 'socialized medicine' and alternatively as 'two-tier healthcare' although I have never seen any real substantiation for the latter charge. My mom had an operation for colon cancer some time back, and she paid nothing for the hospitalization or the operation. My father-in-law is scheduled for the same operation as soon as he gets his blood-sugar low enough, and he already had one for a hernia and removal of internal scar tissue from an old injury – again, we paid nothing. He had a nurse come here for a couple of months, once a week, to change his dressing (because the incision would was very slow to heal because he is diabetic – nothing. That's all great, from my point of view, and I've paid into it all my life without ever using it because I was covered by the government under federal guidelines while I served in the military, although I was a cheap patient because I never had to be hospitalized for anything and was almost never even sick enough not to come to work. But the great drawback to it, as I said, is the backlog which might mean you have to wait too long for an operation. And in my small practical experience – the two cases I have just mentioned – both were scheduled for surgery within a month of diagnosis. So perhaps the long wait is for particular operations such as heart or brain surgery.
The Albanian Kosovo Liberation Army harvested organs from captured Serb civilians and soldiers:et Al , November 28, 2017 at 1:32 amhttps://thebloodyellowhouse.wordpress.com/
In December 14th 2010, Dick Marty, Rapporteur of EU Commission pass for adoption to the Council of Europe a report on allegations of inhuman treatment of people and illicit trafficking in human organs in Kosovo organized by KLA leader and Kosovo Prime minister Hashim Thaçi . An official report accusing Kosovo's prime minister of links to a "mafia-like" network that killed captives in order to sell their organs on the black market was yesterday endorsed by a Council of Europe committee.
Bold text emphasis added.
Nothing came of the charges that I am aware of and it is business as usual with Kosovo and Albania.
Per Wikipedia:
The Washington Times reported that the KLA was financing its activities by trafficking the illegal drugs of heroin and cocaine into western Europe.[16]
A report to the Council of Europe, written by Dick Marty, issued on 15 December 2010[23] states that Hacim Thaçi was the leader of the "Drenica Group" in charge of trafficking organs taken from Serbian prisoners.
On 17 February 2008, Kosovo declared its independence from Serbia. Thaçi became Prime Minister of the newly independent state.
So, there you have it – the war criminal, drug runner, murderer and organ thief/butcher became the PM of Kosovo, a nation created and nurtured by NATO with a nod and a wink from the EU. Simply disgusting but typical treatment for Serbia by the fascist/racist and genocidally inclined West.
Thank you very much for a very interesting article UCG! Quite the horror story. I've heard quite a few about the US over the years from people I know too. I think one of the BBC's former America correspondent gave an interview to the Beeb as he was leaving America a few years back (MAtt Frei?) and was asked what were the best and worst things about living there. The worst was certainly healthcare.yalensis , November 28, 2017 at 3:21 amI've also read that healthcare costs for the self-employed, independents, freelancers can also be crushing in the land of the free where everyone can become rich. Has this changed? I would have thought that those were the ideal Americans, making it off their own back, but apparently not.
There's also another issue that is not addressed: an ageing population. This is a very current theme and it is now not at all unusual for people to live another 30 odd years after retirement. Now how on earth will such people manage their healthcare for such a period? Will they have to hock absolutely everything they have? America is already at war with itself (hence the utmost need to for foreign enemies), but nothing is getting done. Just more of the same. Meanwhile the Brits are trying to copy the US through stealth privatization of their health system. It might work as well as privatizing its rail service
Thanks for an interesting post, UCG. Hopefully this will stimulate some ideas on how to fix the American healthcare system, which seems to be badly broken.Patient Observer , November 28, 2017 at 4:34 amBroken for us but working perfectly for Big Pharma and insurance companies. That is a fundamental reason why it will be extremely difficult to "fix" because it ain't broken as a money making machine.yalensis , November 28, 2017 at 1:25 pmTrue. And the insurance companies, in particular, have been really raking it in, especially with Obamacare and the various Medicare Advantage options.
Nov 30, 2017 | marknesop.wordpress.com
kirill , November 27, 2017 at 8:38 pm
Interesting article. Looks like the rot in the US is terminal. But Canada and its "socialized" medicine is not far behind. Operating an emergency ward with only one doctor doing the rounds at the rest of the hospital during the night is absurd. But that is what major Canadian hospitals do. Don't bother going to emergency at 2 am unless you are literally dying. Wait until 7 am when the day day crew arrives and you can actually receive treatment.Ryan Ward , November 28, 2017 at 3:19 amThe problem in Canada, as in the USA, is overpaid doctors and not enough of them (because they are overpaid). Instead of paying a doctor $300,000 per year or more, the system needs to have 3 or more doctors earning $100,000 per year. Then there is no excuse about being overworked and "requiring" a high compensation. Big incomes attract crooks and not talent. If you want to be a doctor then you should do 5 years of low income work abroad or at home. That would weed out a lot of the $$$ in the eyeballs leeches. A nasty side effect of having overpaid doctors and living adjacent to the US, is that they act like a mafia and extort the government by threatening to leave to the USA. I say that the Canadian provinces should make all medical students sign binding contracts to pay the cost difference between their Canadian medical education and the equivalent in the USA if they decide to run off to America.
At the undergraduate level, the physics courses with the highest enrollment are aimed at streams going into medicine. There are hordes of money maker wannabes trying to make it big in medicine. But they are all nearly weeded out and never graduate from medical school. So the system maintains the fake doctor shortage and racket level salaries. On top of this, hospitals pay a 300% markup for basic supplies (gauze, syringes, etc). It is actually possible for private individuals to pay the nominal price so this is not just a theory. Clearly, there is no effort to control costs by hospital administrations since basic economics would imply that hospitals would pay less than individuals for these items due to the volume of sales involved. At the end of the day North American public medicine is a non-market bloating itself into oblivion since the taxpayer will always pay whatever is desired. That is, the spineless politicians will never crack the whip.
This is part of the problem in Canada. One way to help deal with it in my view, beyond simply cutting doctors' fees (which any government with the political will to do so can do) is to simply make it easier for International Medical Graduates to get licensed in Canada. Canada has legions of immigrants (and could have pretty much however many more it likes) with full medical qualifications who would be thrilled to work for much less than the current pay rates. It's a scandal how many qualified doctors we have in Canada driving taxis rather than practicing medicine. If we just took advantage of the human resources we already have, we could easily say to doctors who threaten to leave for the US, "Fine, go. We've got 10 guys from India lined up to do your job." This isn't to say that doctors shouldn't be very well-paid. Anyone who has ever known someone in med school knows it's hell. But doctors would be very well-paid at half the rates they're getting now.marknesop , November 28, 2017 at 10:32 amAnother part of the problem is an over-reliance on hospitals. There are a lot of people in the hospitals more in "holding" than anything else, because there's no space in the proper facilities for them (The book "Chronic Condition" talks about this). The problem with this is that the cost per day to keep someone in the hospital is much higher than in other kinds of facilities. This is an entirely unnecessary loss.
For all that though, the Canadian system is leaps and bounds better than the American. We spend a vastly smaller percentage of our GDP on health care, and in return achieve higher health outcomes, as measured by the WHO. If we were willing to spend the kind of money the Americans do on health care, we could have patients sleeping in golden beds even with the structural flaws of our current system. That's worth constantly remembering, because some of the proposals for health reform floating around now lean in the direction of privatization, and we've seen where that road leads.
Before he retired from politics, Keith Martin was my MLA, and he was also a qualified MD. He used to rail against the convoluted process for certification in medicine in Canada, while others complained that we were subject to an influx of doctor-immigrants from India because Canada required less time spent in medical school than India does. I never checked the veracity of that, although we do have quite a few Indian doctors. My own doctor – in the military, and still now since he is in private practice – is a South African, and he explained that he had gone in for the military (although he was always a civilian, some military doctors are military members as well but most are not) because the hoop-jumping process to be certified for private practice in Canada with foreign qualifications was just too onerous.Unsurprisingly, I completely agree on the subject of privatization, because it always leads to an emphasis on profit and cost-cutting. I don't know why some people can't see that.
Nov 30, 2017 | marknesop.wordpress.com
kirill , November 27, 2017 at 8:38 pm
Interesting article. Looks like the rot in the US is terminal. But Canada and its "socialized" medicine is not far behind. Operating an emergency ward with only one doctor doing the rounds at the rest of the hospital during the night is absurd. But that is what major Canadian hospitals do. Don't bother going to emergency at 2 am unless you are literally dying. Wait until 7 am when the day day crew arrives and you can actually receive treatment.Ryan Ward , November 28, 2017 at 3:19 amThe problem in Canada, as in the USA, is overpaid doctors and not enough of them (because they are overpaid). Instead of paying a doctor $300,000 per year or more, the system needs to have 3 or more doctors earning $100,000 per year. Then there is no excuse about being overworked and "requiring" a high compensation. Big incomes attract crooks and not talent. If you want to be a doctor then you should do 5 years of low income work abroad or at home. That would weed out a lot of the $$$ in the eyeballs leeches. A nasty side effect of having overpaid doctors and living adjacent to the US, is that they act like a mafia and extort the government by threatening to leave to the USA. I say that the Canadian provinces should make all medical students sign binding contracts to pay the cost difference between their Canadian medical education and the equivalent in the USA if they decide to run off to America.
At the undergraduate level, the physics courses with the highest enrollment are aimed at streams going into medicine. There are hordes of money maker wannabes trying to make it big in medicine. But they are all nearly weeded out and never graduate from medical school. So the system maintains the fake doctor shortage and racket level salaries. On top of this, hospitals pay a 300% markup for basic supplies (gauze, syringes, etc). It is actually possible for private individuals to pay the nominal price so this is not just a theory. Clearly, there is no effort to control costs by hospital administrations since basic economics would imply that hospitals would pay less than individuals for these items due to the volume of sales involved. At the end of the day North American public medicine is a non-market bloating itself into oblivion since the taxpayer will always pay whatever is desired. That is, the spineless politicians will never crack the whip.
This is part of the problem in Canada. One way to help deal with it in my view, beyond simply cutting doctors' fees (which any government with the political will to do so can do) is to simply make it easier for International Medical Graduates to get licensed in Canada. Canada has legions of immigrants (and could have pretty much however many more it likes) with full medical qualifications who would be thrilled to work for much less than the current pay rates. It's a scandal how many qualified doctors we have in Canada driving taxis rather than practicing medicine. If we just took advantage of the human resources we already have, we could easily say to doctors who threaten to leave for the US, "Fine, go. We've got 10 guys from India lined up to do your job." This isn't to say that doctors shouldn't be very well-paid. Anyone who has ever known someone in med school knows it's hell. But doctors would be very well-paid at half the rates they're getting now.marknesop , November 28, 2017 at 10:32 amAnother part of the problem is an over-reliance on hospitals. There are a lot of people in the hospitals more in "holding" than anything else, because there's no space in the proper facilities for them (The book "Chronic Condition" talks about this). The problem with this is that the cost per day to keep someone in the hospital is much higher than in other kinds of facilities. This is an entirely unnecessary loss.
For all that though, the Canadian system is leaps and bounds better than the American. We spend a vastly smaller percentage of our GDP on health care, and in return achieve higher health outcomes, as measured by the WHO. If we were willing to spend the kind of money the Americans do on health care, we could have patients sleeping in golden beds even with the structural flaws of our current system. That's worth constantly remembering, because some of the proposals for health reform floating around now lean in the direction of privatization, and we've seen where that road leads.
Before he retired from politics, Keith Martin was my MLA, and he was also a qualified MD. He used to rail against the convoluted process for certification in medicine in Canada, while others complained that we were subject to an influx of doctor-immigrants from India because Canada required less time spent in medical school than India does. I never checked the veracity of that, although we do have quite a few Indian doctors. My own doctor – in the military, and still now since he is in private practice – is a South African, and he explained that he had gone in for the military (although he was always a civilian, some military doctors are military members as well but most are not) because the hoop-jumping process to be certified for private practice in Canada with foreign qualifications was just too onerous.Unsurprisingly, I completely agree on the subject of privatization, because it always leads to an emphasis on profit and cost-cutting. I don't know why some people can't see that.
Nov 30, 2017 | marknesop.wordpress.com
James lake , November 28, 2017 at 12:21 am
This is s very interesting insight into healcare in the USA. The cost is shocking.marknesop , November 28, 2017 at 10:25 am
I live in the UK and the healthcare system is paid for from taxation.
When it was established over 70 years ago it's
The health service would be available to all and financed entirely from taxation, which meant that people paid into it according to their means.
It was the best thing in my view that government has ever done.
Good healthcare should be available to all and not dependent on peoples ability to pay.However there always a private healthcare system that ran alongside it
And over the years it had been unpicked as successive governments have tried to privatise it. Claiming they will save the taxpayer money
– opticians and dentistry have become part private after 18 if you are employed.
Which many people do not mind.
-Elderly care was also privatised as it's the most expensive
-care for the disabled also is a issue for local councils
-Mental health became care in the community – society's problem!Privatisation has meant profits for businesses, poor services to vulnerable groups.
And yet still more and more taxation is needed for the NHS!
The issue of more money was even part of the Brexit debate as it was stated that leaving the EU would mean more money for the NHS which people are proud of.There was a quote I was thinking of using in the lead-in, but decided in the end not to since I didn't want to have too many and it might have become confusing. It related that you would get the best medical care of your lifetime – after you died, when they were rushing to save your organs, for transplant. Obviously this would not be true if you were not an organ donor (at least in this country) or died as the result of general wasting away so that you had nothing left which would be particularly coveted. But this is a major issue in medicine in some countries and there have been various lurid tales of bodies being robbed of their organs without family permission, bodies of Ukrainian soldiers harvested of their organs and rackets in third-world countries where the poor or helpless are robbed of organs while they are alive. From my standpoint, since I haven't done much research on it, I have seen little proof of any of them despite plenty of allegation, but it is easy to understand that traffic in organs to those who will pay anything to live a little longer would be tremendously profitable, and the potential for disproportionate profit seldom fails to draw the unscrupulous.Patient Observer , November 28, 2017 at 12:49 pmAs I alluded in the lead-in, Canada has what is sometimes described as 'socialized medicine' and alternatively as 'two-tier healthcare' although I have never seen any real substantiation for the latter charge. My mom had an operation for colon cancer some time back, and she paid nothing for the hospitalization or the operation. My father-in-law is scheduled for the same operation as soon as he gets his blood-sugar low enough, and he already had one for a hernia and removal of internal scar tissue from an old injury – again, we paid nothing. He had a nurse come here for a couple of months, once a week, to change his dressing (because the incision would was very slow to heal because he is diabetic – nothing. That's all great, from my point of view, and I've paid into it all my life without ever using it because I was covered by the government under federal guidelines while I served in the military, although I was a cheap patient because I never had to be hospitalized for anything and was almost never even sick enough not to come to work. But the great drawback to it, as I said, is the backlog which might mean you have to wait too long for an operation. And in my small practical experience – the two cases I have just mentioned – both were scheduled for surgery within a month of diagnosis. So perhaps the long wait is for particular operations such as heart or brain surgery.
The Albanian Kosovo Liberation Army harvested organs from captured Serb civilians and soldiers:et Al , November 28, 2017 at 1:32 amhttps://thebloodyellowhouse.wordpress.com/
In December 14th 2010, Dick Marty, Rapporteur of EU Commission pass for adoption to the Council of Europe a report on allegations of inhuman treatment of people and illicit trafficking in human organs in Kosovo organized by KLA leader and Kosovo Prime minister Hashim Thaçi . An official report accusing Kosovo's prime minister of links to a "mafia-like" network that killed captives in order to sell their organs on the black market was yesterday endorsed by a Council of Europe committee.
Bold text emphasis added.
Nothing came of the charges that I am aware of and it is business as usual with Kosovo and Albania.
Per Wikipedia:
The Washington Times reported that the KLA was financing its activities by trafficking the illegal drugs of heroin and cocaine into western Europe.[16]
A report to the Council of Europe, written by Dick Marty, issued on 15 December 2010[23] states that Hacim Thaçi was the leader of the "Drenica Group" in charge of trafficking organs taken from Serbian prisoners.
On 17 February 2008, Kosovo declared its independence from Serbia. Thaçi became Prime Minister of the newly independent state.
So, there you have it – the war criminal, drug runner, murderer and organ thief/butcher became the PM of Kosovo, a nation created and nurtured by NATO with a nod and a wink from the EU. Simply disgusting but typical treatment for Serbia by the fascist/racist and genocidally inclined West.
Thank you very much for a very interesting article UCG! Quite the horror story. I've heard quite a few about the US over the years from people I know too. I think one of the BBC's former America correspondent gave an interview to the Beeb as he was leaving America a few years back (MAtt Frei?) and was asked what were the best and worst things about living there. The worst was certainly healthcare.yalensis , November 28, 2017 at 3:21 amI've also read that healthcare costs for the self-employed, independents, freelancers can also be crushing in the land of the free where everyone can become rich. Has this changed? I would have thought that those were the ideal Americans, making it off their own back, but apparently not.
There's also another issue that is not addressed: an ageing population. This is a very current theme and it is now not at all unusual for people to live another 30 odd years after retirement. Now how on earth will such people manage their healthcare for such a period? Will they have to hock absolutely everything they have? America is already at war with itself (hence the utmost need to for foreign enemies), but nothing is getting done. Just more of the same. Meanwhile the Brits are trying to copy the US through stealth privatization of their health system. It might work as well as privatizing its rail service
Thanks for an interesting post, UCG. Hopefully this will stimulate some ideas on how to fix the American healthcare system, which seems to be badly broken.Patient Observer , November 28, 2017 at 4:34 amBroken for us but working perfectly for Big Pharma and insurance companies. That is a fundamental reason why it will be extremely difficult to "fix" because it ain't broken as a money making machine.yalensis , November 28, 2017 at 1:25 pmTrue. And the insurance companies, in particular, have been really raking it in, especially with Obamacare and the various Medicare Advantage options.
Nov 30, 2017 | marknesop.wordpress.com
Ryan Ward , November 28, 2017 at 3:40 am
With health care in general, there's a bit of a trade-off. The most cost-efficient systems, like the system in Sweden for example, are fairly regimented and don't leave much room for individual choice (unless someone pays out of pocket for treatment completely outside the public system). On the other hand, systems that give people a little more choice, like the system in Germany, tend to be a little on the pricey side. I think, given American political culture, something along the lines of the German model is much more likely to attract widespread public support. In any case, it's still cheaper than the American system, and achieves some of the best results in the world. https://en.wikipedia.org/wiki/Healthcare_in_Germany
Nov 30, 2017 | marknesop.wordpress.com
[email protected] , November 27, 2017 at 6:02 pm
I find it terribly silly that we should even consider med student's debt as an excuse. First, American doctors are the best paid professionals in the country. Internists make a median 190 thousand a year, and they are among the worst paid specialties. I cannot possibly see the problem with paying your income for 5 years, knowing that you get access to a caste that will allow you make good money into your eighties.ucgsblog , November 28, 2017 at 4:08 pmSecond, the debt is not that high as you claim. Harvard Medical School tuition is 64 thousand. You can rent across the street with 20 thousand a year – I currently live there.
Third, med students know all this. The reason why they borrow far more is because they know they can afford it. I went to med school somewhere in a developing world. We shared toilets in the dorm. As a matter of fact, most under-30s in Boston live in shared accommodation. The outliers? Med students. Even the lowly Tufts and BU students that I met own cars and live by themselves, mainly in new buildings across the street from their hospitals.
Every time I go to the doctors, I am thinking how I am going to sue their asses if they make a mistake.
It's not an excuse. It's a bill. When you rent an apartment, did you know that most landlords also factor in the property tax when figuring out what your rent payment should be? Similarly, the interest payments on the doctoral students' loans are passed off to the consumer, and that is yet another reason why Healthcare is so expensive. That's why I think that medical school should be free for those students who promise to charge their patients no more than x amount of money.
Nov 30, 2017 | marknesop.wordpress.com
Patient Observer , November 27, 2017 at 5:12 pm
Mark, today's posting provided is a nice change of pace to a topic of local impact (for me at least). UGC presented a good overview peppered with supporting data.marknesop , November 28, 2017 at 12:10 amIn an earlier career incarnation, I worked as a systems analyst involved with development of online systems for state social services. Data showed that our systems were able to administer a comprehensive health care program for social services recipients for about 3-4% of the cost of services. Private medical insurance providers required approximately 20% of the cost of services to provide similar services. Yet, private providers were supposedly driven by invisible market forces to maximum efficiency. BS. In fact, they are driven by greed and they found it much easier to maximize profits by colluding with politicians and health care providers. That is the trouble with free markets – its just so damn easy to cheat and cheaters are never in short supply.
One more thing, prescription drugs costs may exceed $600 billion in the US by 2021:
That would be nearly $2,000 per year for every American!
If a tiny fraction of that amount were spent on prevention, education, improved diets and other similar initiatives, the population ought to be healthier and richer. But, greed overpowers the public good every time. The US health care system is a criminal enterprise in my opinion. The good that it does is grossly outweighed by greed and exploitation of human suffering.
I believe the author is also a systems analyst, so you are thinking along similar lines.ucgsblog , November 28, 2017 at 4:05 pmI agree with that. Plus, it seems like they have an entire staff dedicated to giving their "customer" the run around. A friend of mine had to deal with several different departments regarding his healthcare bill. The billing office told him that they only deal with billing questions, and that for explanations for the bill, he should call the doctor's office. The doctor's office told him to call the hospital, since that's where the service took place. The hospital told him to call his primary doctor, who sent him there, and his primary doctor referred him back to the specialist, where he was referred back to the billing department, which promptly told him that they're closing for the day, since he spent 6 hours being transferred from one department to the next.
Nov 27, 2017 | marknesop.wordpress.com
"The art of medicine consists of amusing the patient while nature cures the disease."
"No, I mean I'm sorry that you've inherited such a miserable, collapsing Old Country. A place where rich Bankers own everything, where you've got to be grateful for a part-time job with no benefits and no retirement plan, where the most health insurance you can afford is being careful and hoping you don't get sick
Cory Doctorow; Homeland
"Until fairly recently, every family had a cornucopia of favorite home remedies–plants and household items that could be prepared to treat minor medical emergencies, or to prevent a common ailment becoming something much more serious. Most households had someone with a little understanding of home cures, and when knowledge fell short, or more serious illness took hold, the family physician or village healer would be called in for a consultation, and a treatment would be agreed upon. In those days we took personal responsibility for our health–we took steps to prevent illness and were more aware of our bodies and of changes in them. And when illness struck, we frequently had the personal means to remedy it. More often than not, the treatment could be found in the garden or the larder. In the middle of the twentieth century we began to change our outlook. The advent of modern medicine, together with its many miracles, also led to a much greater dependency on our physicians and to an increasingly stretched healthcare system. The growth of the pharmaceutical industry has meant that there are indeed "cures" for most symptoms, and we have become accustomed to putting our health in the hands of someone else, and to purchasing products that make us feel good. Somewhere along the line we began to believe that technology was in some way superior to what was natural, and so we willingly gave up control of even minor health problems."
Karen Sullivan; The Complete Family Guide to Natural Home Remedies: Safe and Effective Treatments for Common Ailments
No, I haven't abandoned Uncle Volodya, or shifted my focus to American administration; what follows is a guest post on the American healthcare system, by our friend UCG. As I've mentioned before – on the occasion of his previous guest post, in fact – he is an ethnic Russian living in the Golden State.
As an American in America, naturally his immediate concern is going to be healthcare in America; but there are lessons within for everyone. Don't get me wrong – doctors have done a tremendous amount of good, and medical researchers and many others from the world of medicine have made tremendous advances to which many of us owe their lives. Sadly, though, once a field goes commercial, the main focus of attention eventually becomes profit, and there are few endeavors in which the customer base will be so desperate. While there are obvious benefits to 'socialized medicine' such as Canada enjoys and American politicians scorn as 'Commie' – enough to earn the admiration of many – it results in such a backlog for major operations that those who don't like their chances of dying first, and have the money or can somehow get it, often flee to America, where you can get a good standard of medical care without running out of time waiting for it.
Without further ado, take it away, UCG!!
Healthcare in America
This article is my opinion. My hope is that others will do their own research on America's Healthcare Industry, because this is an issue that needs to be addressed, and for this article to be a mere starting point in this research. The reason for my citations is so that you, the reader, can verify them. Once again, this is my opinion. I write this in the first paragraph, so that I can avoid stating "in my opinion" before every sentence.
Let's start with Owen Davis who was charged $14,018 for going to a hospital because he sliced his hand, and they fixed it . A study published by Johns Hopkins showed that for $100 of ER treatment, some hospitals were charging patients up to $1,260 . A redditor claimed that :
I tore my ab wall a month ago and didn't think much of it until my pain kept worsening. I went to an immediate care facility to rule out a hernia (I had all the symptoms) and they told me to get to ER ASAP. I go to the ER and they give me a CT scan and one x-ray and say it's not a hernia and let me go. Fast forward to today and I got a bill for $9,200 and $3,900 of it is out of pocket. $9,200 for two tests???? No pain meds were administered; it was literally those two tests. What should I do to contest it? I will be calling tomorrow to demand an itemized bill, but is there anything else I should do in the meantime?
All of these took me a few minutes on Google to find, and another few minutes to post. The reason I chose that reddit, is because one of the readers offered an ingenious solution: Next time you hurt yourself – book a return ticket to NZ – go to accident and emergency, say you're a tourist and you hurt yourself surfing, pay nothing – fly home and pocket $8,000 in spare change. If that was me, I'd spend at least $2,000 on tourism in New Zealand. You guys have that system, so you clearly deserve the money! Anyone interested in a startup?
But I am not done with examples just yet. Shana Sweney described her experience in the emergency room : I delivered in 15 minutes. During that time, the anesthesiologist put a heart rate monitor on my finger and played on his phone. My bill for his services was $3,000. $200/minute. I talked to the insurance company about it – and since I ran my company's benefit plans, I got a little further than most people, but ultimately, that was what their contract with the hospital said so that's what they had to pay. Regardless of if he worked 15 minutes or 3 hours. Similarly, my twins were born prematurely and ended up in the NICU for 2 weeks. While the NICU was in-network for my insurance, for some mysterious reason, the neonatologists that attended the NICU were out of network. I think that bill was $16k and they stopped by to see each kid for an average of about 30 min/day.
Almost done with the examples, just please bear with me. How would you like a hospital billing you $83,046 for treating a scorpion sting , if a Mexican ER might have treated you for the same type of sting for $200? Perhaps being charged $546 for six liters of saltwater is more to your liking? $1,420 for two hours of babysitting ? $55,000 for an appendicitis operation ? $144,000 to deliver a perfectly healthy, albeit quite impatient baby? According to my interpretation of the sources linked, all of these actually happened. I encourage you to do your own research.
The World's Biggest Legalized Corruption (IMHO)
$984.157 billion. That's $984,157,000,000. That is how much money I believe the United States wastes on Healthcare. Not spends; wastes. As in money down the drain. The astute reader figured out that equates to five percent of America's 2016 GDP . Said reader is absolutely correct. How did I estimate such a gargantuan amount? According to the OECD data , in 2013 the United States spent 16.4 percent of its GDP on Healthcare; the two next biggest spenders, Switzerland and the Netherlands spent 11.1 percent. Even if one was to give the United States the benefit of doubt, and claim that the United States healthcare is just as efficient as that of Switzerland or the Netherlands – which is most likely not true according to an article from Business Insider , but even if it was – that meant that the United States wastes 5.3% of its GDP on healthcare. Wastes. I just want to make sure that the amount of this alleged legalized corruption, which will most likely reach a trillion dollars by 2020, is noted.
Let me place those funds into perspective: it's almost as much as the amount that the rest of the World spends on the military, combined . The SCO member states, including China, Russia, India, and Pakistan spent roughly $360 billion on the military . The wasted amount is equivalent to the GDP of Indonesia, and greater than the GDP of Turkey or Switzerland . In 2016, the US Federal Government spent $362 billion, or 36.8% of the wasted amount, to run all Federal Programs , including the Department of Education and NASA, with the exception of Social Security, Medicare/Medicaid, Veteran's Affairs, the military, and net interest on the US debt. All other Federal Programs were covered with the $362 billion. The US Federal Debt stands at $20.4 trillion , meaning that the debt can be paid off in 30 years, merely if the Healthcare Waste is eliminated.
But why stop there? The US Housing Crisis started partly because loans were allowed to be taken out without the 20% down payment. Could this funding, if applied directly to the housing market, stop the 2008 Great Recession? Absolutely, and all the Federal Government had to do was to gear these funds towards down payment on subprime mortgage loans to meet the 20 percent barrier. I can go on and on about what can be accomplished, like making collegiate attendance free, or at least very inexpensive, or drastically improving the quality of education, paying off the national debt, reinvesting into the economy, reinvigorating the rural sector, and so on, and so forth. A trillion dollars is a lot of money.
Lobbyists, the Media and the Waste
Any guess how much was spent on lobbying by the Healthcare, Insurance, Hospitals, Health Professionals, and HMOs? How about 10.5 billion dollars? I knew that was your guess! That's a lot of money, and that does not include "speaking fees", or when a politician who constantly made calls beneficial to the Healthcare Lobby gets $150,000 to speak in front of an audience after they retire from politics. Obama made a speech in front of Wall Street, netting $400,000 . And by pure coincidence, only one Wall Street Broker was jailed as a result of the scandal. That $10.5 billion is just a tip of the iceberg, because "speaking fees" are notoriously hard to track, and not included in said amount.
Obama genuinely tried to reform US Healthcare to the Swiss Model. He was going to let Wall Street slide, he was going to let Neocons conduct foreign policy, just please, let him have healthcare! First, the lobbyists laughed in his face. Second, they utilized the Blue Dog Coalition to block Obama's attempt at Healthcare Reform, until it was phenomenally nerfed, and we have the disaster that we have today. As a result, Obama's Legacy, Obamacare is having major issues, including the rise of racism.
Obamacare helped the poor, (mostly minorities,) at the expense of the middle class, (mostly whites,) thus transferring funding from whites to minorities. While the intent was not racial, it is being called out as racial by the mainstream media . This probably suits the lobbyists, because if the debate is about racism, one cannot have a genuine discussion about Healthcare Reform.
Racism strikes both ways. Samantha Bee came out with a "fuck you white people" message right after the election. Jon Stewart, without whom she probably wouldn't have her own show, pointed out that it was simply economics, like the healthcare insurance premium increase , that brought Donald Trump to power. Interestingly enough, James Carville made the same argument when Bill Clinton beat George Bush, but when Hillary Clinton lost, Carville was quick to blame Russia. These delusions on the Left are letting the Right mobilize stronger than ever before. And all of this takes away from the Healthcare Debate.
In an attempt to blame Trump's Election on white racism, rather than basic economics, numerous outlets simply fell flat. For instance, Eric Sasson writes : white men went 63 percent for Trump versus 31 percent for Clinton, and white women went 53-43 percent. Among college-educated whites, only 39 percent of men and 51 percent of women voted for Clinton What's more, these people hadn't suffered under Obama; they'd thrived. The kind of change Trump was espousing wasn't supposed to connect with this group.
Did this group thrive? The collegiate debt went from $600 billion to $1.4 trillion under Obama's Administration, while the health insurance increased from $13,000 to $18,000 per family . This is thriving? Was the author experimenting with medical marijuana when said article was written? Nevertheless, the parade of insanity continued, with Salon assuring us that it was blatant racism that gave us Trump . The Root, which also claimed that Russians attempted to hack election machines, pointed out that Russia exploited America's racism , and thus Trump won the election. Washington Post claimed that racism motivated white people more than authoritarianism . Comedian Bill Maher tried to sway the discussion back to economics, by pointing out that outrage over Pocahontas or Halloween should not stop the Democrats from working for the working man . Sadly, Maher and Stewart are in the minority, and instead of a Healthcare Debate, the US is now stuck in a debate over racism, which isn't even three-fifths as effective. Meanwhile the US continues to waste almost a trillion dollars on healthcare .
Who Benefits?
Let's start with the banks. Medical students graduate with an average of $416,216 in student debt . The average interest rate on said loan is seven percent. Roughly 20,055 students go through this program, per year . Presuming a twenty year loan, the banks are looking at about $7.185 billion in interest payments. It really is a small fraction of the cost. Prescription drug prices are another story. In 2014, Medicare spent $112 billion on medicine for the elderly . Oh la la! Cha-ching. I would not be surprised if at least half of that was wasted on drug price inflation. You know the health insurance companies? It's a great time to be one, since profits are booming – to the tune of $18 billion in projected revenue for 2017.
Of course the system itself is quite wasteful, with needless hours spent on paperwork, claim verification, contractual review, etc, etc, etc. Humana's revenue was $54.4 billion , Aetna's was $63.2 billion , Anthem's was $85 billion , Cigna's was $39.7 billion , and UnitedHealth's was $184.8 billion . Those are just the top five companies. None of them ia a mom-and-pop shop or small business store. Do any of these insurers support Obamacare? Even if they do, it is without much enthusiasm . They are leaving, and leaving quite quickly. Thirty-one percent of American counties will have just one healthcare insurer . Welcome to a monopoly that is artificially creating itself. And despite the waste, 28.2 million Americans remain uninsured . Mission accomplished!
Who else benefits? Those who hire illegal immigrants instead of American workers, since illegal immigrants cost the United States roughly $25 billion in Healthcare spending . Meanwhile those who hire them can avoid certain types of taxes and not have to cover their Healthcare; communism for the rich, capitalism for the rest of us. Of course that is just a rough estimate, since this spending is also quite hard to track.
The Future
The problem with changing Healthcare is that too many people have their hands in the proverbial pie. There is not a single lever of power that isn't affected by Healthcare, and most of the levers that are affected, benefit quite a bit. Insurance companies will fight to the death, because Universal Healthcare will be their death knell. Banks will defend it, because who doesn't want to make billions from student loans? Medical schools too – since it lets them charge higher and higher tuition. Pharmaceutical companies can use the increase in Healthcare expenditure to justify their own price hikes, even though a major reason for those price hikes is artificial patent based monopoly.
What is an artificial monopoly? In my opinion, it's when a patent is utilized to prevent competitors from manufacturing the same exact drug. In less than a decade, the price of Epi-Pen soared from $103.50 to $608.61. When asked the justify said increase, one of the reasons provided by the CEO was that the price went up because we were making investment; as I said, about $1 billion over the last decade that we invested in the product that we could reach physicians and educate legislatures. "Reaching" doctors and legislators; I wonder, how was said "education funding" spent? According to US News, a website that is extremely credible when it comes to internal decision making within the United States, drug companies have long courted doctors with gifts , from speaking and consulting fees to educational materials to food and drink. But while most doctors do not believe these gifts influence their decisions about which drugs to prescribe, a new study found the gifts actually can make a difference – something patient advocates have voiced concern about in the past. Do you feel educated? Would you feel more educated if I paid you a $150,000 consulting fee? What about $400,000? What? It's just consulting; no corruption here!
Everyone knows that this is going on. But there is not going to be change. Why not? The same reason that there was not change with Harvey Weinstein, until Taylor Swift came along. Remember how I said that almost everyone has their hands in the Healthcare Pie? It was not much different with Weinstein. Scott Rosenberg explained why it took so long for people to speak out against Harvey , and the reasons were numerous. First, Harvey gave many people their start in Hollywood, and treated all of his friends like royalty. That drastically increased their loyalty. Second, he ushered the Golden Age of the 1990s, with movies like Pulp Fiction, Shakespeare in Love, Clerks, Swingers, Scream, Good Will Hunting, English Patient, Life is Beautiful – the man could make phenomenal movies. Third, even if one was willing to go against his own friends, workers, mass media, and so on, there was no one to tell. There was no place to speak out. Fourth, some of the victims took hefty settlements.
That fourth reason enabled mass media to portray rape victims as gold diggers. Rape Culture is alive and well. In California, a Judge gave minimal sentencing to a convicted rapist , because he was afraid a harsher sentence would damage the rapist's mental psyche for life. Uh dude, from one Californian to another, he, uh, raped. His mental psyche is already damaged; for life. That's the kind of pressure that Rose McGowan had to deal with. She had a little kerfuffle with Amazon , and she thinks it was partially because of Harvey Weinstein. How many times had the word "socialism" been thrown around to describe Universal Healthcare? Switzerland has it – are they Socialist?
Enter Taylor Swift . In order to destroy allegations that women are filing sexual harassment claims as gold diggers, she sued her alleged sexual assaulter for a buck; one dollar. She won. Swift stated that the lawsuit was to serve as an example to other women who may resist publicly reliving similar outrageous and humiliating acts. On top of that, Weinstein was no longer as popular as he used to be, and an avenue to tell the story, an outlet was created. The additional prevalence of the internet caused the stories of Weinstein's sexual abuse to leak. Within a month, the giant fell.
Something similar is needed to change Healthcare in America. But until that comes along, racism will increase, the cost of Healthcare will rise, emergency room costs will most likely double every ten years, and the future remains bleak. As if that was not enough, more and more upper class Americans, (like yours truly,) are seeking treatment abroad. It cost me less money to lose five weeks of wages, spend three weeks partying in Eastern Europe, (Prague to be more specific,) after my two weeks of treatment, buy a roundtrip plane ticket, and stay in a five star, all-inclusive hotel, than the cost of the same treatment in the US. If anyone wants to utilize this as a startup – let me know!
Of course its effects on Healthcare will hurt, since it is a huge chunk of business that will be traveling across the Atlantic. But what can be done to stop it? One cannot stop Americans from traveling to other countries. One cannot force the poor to work for free. Perhaps this is the change that is needed to make those who benefit from the Healthcare Waste realize that this cannot continue. Perhaps not. What we do know, is that Obamacare insured the poor, at the expense of the middle class . And that is regarded as a failure in America.
Northern Star , November 27, 2017 at 3:12 pmAs for Obongo Care ??:ucgsblog , November 28, 2017 at 3:58 pm"In trying to show that he was successfully managing the Obamacare rollout, the president last week staged a high-profile White House meeting with private health insurance executives -- aka Obamacare's middlemen. The spectacle of a president begging these middlemen for help was a reminder that Obamacare did not limit the power of the insurance companies as a single-payer system would.
****The new law instead cemented the industry's profit-extracting role in the larger health system -- and it still leaves millions without insurance."*** (THAT is the Achille's lower torso of the ACA)https://www.healthcare-now.org/blog/single-payer-healthcare-vs-obamacare/
Exactly! That's why I stated that they're now oligapolizing the market, and will slowly start to increase their insurance rates and profits once again.Northern Star , November 27, 2017 at 3:23 pm"Prince Harry..Do you take this American mulatto negress -aka raghead untermensch-as your lawfully wedded royal wife?*Northern Star , November 27, 2017 at 3:52 pm
http://www.newsweek.com/prince-harrys-worst-moments-meghan-markle-rogue-723177
https://www.sbs.com.au/guide/sites/sbs.com.au.guide/files/styles/body_image/public/nazi.jpg?itok=q1oxMi44&mtime=1503879842Ummm Advice to Meghan .make sure the honeymoon motorcade stays clear of tunnels in Paris
or elsewhere!!!Appurtenant to many of the issues raised in Mark's post:Patient Observer , November 27, 2017 at 5:17 pmhttp://www.wsws.org/en/articles/2017/11/27/pers-n27.html
(Socialist or not..the WSWS writers continue to state that which NEEDS to be hammered home)
"The vast wealth of the financial oligarchy, expressed in their ownership of massive corporations, must be seized and expropriated, while the complex technologies, supply chains, and advanced transportation systems must be integrated in an organized, planned manner to harness the anarchic force of the world economy and eliminate material scarcity.
Amazon is a prime example. Its supply lines and delivery systems could distribute goods across the world, bringing water, food, and medicine from each producer according to his or her ability, to each consumer according to his or her need.
The massively sophisticated computational power used by the technology companies to censor and blacklist political opposition could instead be used for logistical analysis to conduct rescue and rebuilding missions in disaster zones like Houston and Puerto Rico. Drones used in the battlefield could be scrapped and rebuilt to distribute supplies for building schools, museums, libraries, and theaters, and for making Internet service available at no cost for the entire world.
The ruling class and all of the institutions of the political establishment stand inexorably in the way of efforts to expropriate their wealth. What is required is to mobilize the working class in a political struggle against the state and the socio-economic system on which it is based, through the fight for socialism.
Eric London "Particularly for American Stooges:
Advanced technology is helpful but not essential for a humane and just society. Its what we believe and feel that matters. FWIW, I like socialism on a national/international level and individual accountability on a personal level.saskydisc , November 27, 2017 at 4:04 pmWhile general medical care is single payer in Canada, dental services are not. For major work on teeth, it is cheaper to fly to Mexico. The downside is for Mexicans -- such practices will drive the costs up in Mexico.Patient Observer , November 27, 2017 at 5:12 pmMark, today's posting provided is a nice change of pace to a topic of local impact (for me at least). UGC presented a good overview peppered with supporting data.marknesop , November 28, 2017 at 12:10 amIn an earlier career incarnation, I worked as a systems analyst involved with development of online systems for state social services. Data showed that our systems were able to administer a comprehensive health care program for social services recipients for about 3-4% of the cost of services. Private medical insurance providers required approximately 20% of the cost of services to provide similar services. Yet, private providers were supposedly driven by invisible market forces to maximum efficiency. BS. In fact, they are driven by greed and they found it much easier to maximize profits by colluding with politicians and health care providers. That is the trouble with free markets – its just so damn easy to cheat and cheaters are never in short supply.
One more thing, prescription drugs costs may exceed $600 billion in the US by 2021:
That would be nearly $2,000 per year for every American!
If a tiny fraction of that amount were spent on prevention, education, improved diets and other similar initiatives, the population ought to be healthier and richer. But, greed overpowers the public good every time. The US health care system is a criminal enterprise in my opinion. The good that it does is grossly outweighed by greed and exploitation of human suffering.
I believe the author is also a systems analyst, so you are thinking along similar lines.ucgsblog , November 28, 2017 at 4:05 pmI agree with that. Plus, it seems like they have an entire staff dedicated to giving their "customer" the run around. A friend of mine had to deal with several different departments regarding his healthcare bill. The billing office told him that they only deal with billing questions, and that for explanations for the bill, he should call the doctor's office. The doctor's office told him to call the hospital, since that's where the service took place. The hospital told him to call his primary doctor, who sent him there, and his primary doctor referred him back to the specialist, where he was referred back to the billing department, which promptly told him that they're closing for the day, since he spent 6 hours being transferred from one department to the next.[email protected] , November 27, 2017 at 6:02 pmI find it terribly silly that we should even consider med student's debt as an excuse. First, American doctors are the best paid professionals in the country. Internists make a median 190 thousand a year, and they are among the worst paid specialties. I cannot possibly see the problem with paying your income for 5 years, knowing that you get access to a caste that will allow you make good money into your eighties.ucgsblog , November 28, 2017 at 4:08 pmSecond, the debt is not that high as you claim. Harvard Medical School tuition is 64 thousand. You can rent across the street with 20 thousand a year – I currently live there.
Third, med students know all this. The reason why they borrow far more is because they know they can afford it. I went to med school somewhere in a developing world. We shared toilets in the dorm. As a matter of fact, most under-30s in Boston live in shared accommodation. The outliers? Med students. Even the lowly Tufts and BU students that I met own cars and live by themselves, mainly in new buildings across the street from their hospitals.
Every time I go to the doctors, I am thinking how I am going to sue their asses if they make a mistake.
It's not an excuse. It's a bill. When you rent an apartment, did you know that most landlords also factor in the property tax when figuring out what your rent payment should be? Similarly, the interest payments on the doctoral students' loans are passed off to the consumer, and that is yet another reason why Healthcare is so expensive. That's why I think that medical school should be free for those students who promise to charge their patients no more than x amount of money.kirill , November 27, 2017 at 8:38 pmInteresting article. Looks like the rot in the US is terminal. But Canada and its "socialized" medicine is not far behind. Operating an emergency ward with only one doctor doing the rounds at the rest of the hospital during the night is absurd. But that is what major Canadian hospitals do. Don't bother going to emergency at 2 am unless you are literally dying. Wait until 7 am when the day day crew arrives and you can actually receive treatment.Ryan Ward , November 28, 2017 at 3:19 amThe problem in Canada, as in the USA, is overpaid doctors and not enough of them (because they are overpaid). Instead of paying a doctor $300,000 per year or more, the system needs to have 3 or more doctors earning $100,000 per year. Then there is no excuse about being overworked and "requiring" a high compensation. Big incomes attract crooks and not talent. If you want to be a doctor then you should do 5 years of low income work abroad or at home. That would weed out a lot of the $$$ in the eyeballs leeches. A nasty side effect of having overpaid doctors and living adjacent to the US, is that they act like a mafia and extort the government by threatening to leave to the USA. I say that the Canadian provinces should make all medical students sign binding contracts to pay the cost difference between their Canadian medical education and the equivalent in the USA if they decide to run off to America.
At the undergraduate level, the physics courses with the highest enrollment are aimed at streams going into medicine. There are hordes of money maker wannabes trying to make it big in medicine. But they are all nearly weeded out and never graduate from medical school. So the system maintains the fake doctor shortage and racket level salaries. On top of this, hospitals pay a 300% markup for basic supplies (gauze, syringes, etc). It is actually possible for private individuals to pay the nominal price so this is not just a theory. Clearly, there is no effort to control costs by hospital administrations since basic economics would imply that hospitals would pay less than individuals for these items due to the volume of sales involved. At the end of the day North American public medicine is a non-market bloating itself into oblivion since the taxpayer will always pay whatever is desired. That is, the spineless politicians will never crack the whip.
This is part of the problem in Canada. One way to help deal with it in my view, beyond simply cutting doctors' fees (which any government with the political will to do so can do) is to simply make it easier for International Medical Graduates to get licensed in Canada. Canada has legions of immigrants (and could have pretty much however many more it likes) with full medical qualifications who would be thrilled to work for much less than the current pay rates. It's a scandal how many qualified doctors we have in Canada driving taxis rather than practicing medicine. If we just took advantage of the human resources we already have, we could easily say to doctors who threaten to leave for the US, "Fine, go. We've got 10 guys from India lined up to do your job." This isn't to say that doctors shouldn't be very well-paid. Anyone who has ever known someone in med school knows it's hell. But doctors would be very well-paid at half the rates they're getting now.marknesop , November 28, 2017 at 10:32 amAnother part of the problem is an over-reliance on hospitals. There are a lot of people in the hospitals more in "holding" than anything else, because there's no space in the proper facilities for them (The book "Chronic Condition" talks about this). The problem with this is that the cost per day to keep someone in the hospital is much higher than in other kinds of facilities. This is an entirely unnecessary loss.
For all that though, the Canadian system is leaps and bounds better than the American. We spend a vastly smaller percentage of our GDP on health care, and in return achieve higher health outcomes, as measured by the WHO. If we were willing to spend the kind of money the Americans do on health care, we could have patients sleeping in golden beds even with the structural flaws of our current system. That's worth constantly remembering, because some of the proposals for health reform floating around now lean in the direction of privatization, and we've seen where that road leads.
Before he retired from politics, Keith Martin was my MLA, and he was also a qualified MD. He used to rail against the convoluted process for certification in medicine in Canada, while others complained that we were subject to an influx of doctor-immigrants from India because Canada required less time spent in medical school than India does. I never checked the veracity of that, although we do have quite a few Indian doctors. My own doctor – in the military, and still now since he is in private practice – is a South African, and he explained that he had gone in for the military (although he was always a civilian, some military doctors are military members as well but most are not) because the hoop-jumping process to be certified for private practice in Canada with foreign qualifications was just too onerous.Jen , November 27, 2017 at 11:15 pmUnsurprisingly, I completely agree on the subject of privatization, because it always leads to an emphasis on profit and cost-cutting. I don't know why some people can't see that.
Thanks very much UCG, for your article. Very interesting reading for us Australians as the Federal Government eventually wants to shove us kicking and screaming into a US-style privatised healthcare insurance model.Fern , November 28, 2017 at 7:02 amFunnily enough I'm currently considering changing my private health insurer. I'm with Medibank Private at present but considering maybe going with a smaller non-profit health fund like Australian Unity or Phoenix Health Fund.
I was just about to post along the lines of "I don't know if Jen has experienced this in Australia but here in the UK ." so I'll finish the thought. In the UK, successive governments, not just Conservative ones, have been trying to dismantle the NHS and move us to the American system. It is pure ideology – no amount of the very abundant evidence of the inefficiencies of the US system, its waste etc makes any dint in the enthusiasm of those pressing for change.ucgsblog , November 28, 2017 at 4:17 pmThank you Jen! My advice: don't let the Government cajole you into wasting your money on Corporate Greed. Share the article with your fellow Australians, if you must, but don't let our wasteful system be replicated. Interestingly enough, one of my friends, Lytburger, send me a meme right after Ukraine adopted America's Healthcare System, it said: "ISIS refused to take responsibility for Ukraine's Healthcare Reform!" I'd be happy to provide other data or answer questions about the Healthcare System here.James lake , November 28, 2017 at 12:21 amAs for insurance, I'm not sure if Australia has the in-network and out-of-network rules. Does it? Whatever insurance you get, make sure that it has good coverage. If you own a home in the US, and you end up in a hospital's emergency room that's not covered by your insurance, the hospital can take your house under certain circumstances. Ironically, even the Government cannot. All of my real property is in various Trust Accounts, just in case, and I make sure that I have insurance where all major hospitals are in-network and that's the best I can do.
This is s very interesting insight into healcare in the USA. The cost is shocking. I live in the UK and the healthcare system is paid for from taxation. When it was established over 70 years ago it's. The health service would be available to all and financed entirely from taxation, which meant that people paid into it according to their means. It was the best thing in my view that government has ever done. Good healthcare should be available to all and not dependent on peoples ability to pay.marknesop , November 28, 2017 at 10:25 amHowever there always a private healthcare system that ran alongside it
And over the years it had been unpicked as successive governments have tried to privatise it. Claiming they will save the taxpayer money
– opticians and dentistry have become part private after 18 if you are employed.
Which many people do not mind.
-Elderly care was also privatised as it's the most expensive
-care for the disabled also is a issue for local councils
-Mental health became care in the community – society's problem!
Privatisation has meant profits for businesses, poor services to vulnerable groups.
And yet still more and more taxation is needed for the NHS!
The issue of more money was even part of the Brexit debate as it was stated that leaving the EU would mean more money for the NHS which people are proud of.
There was a quote I was thinking of using in the lead-in, but decided in the end not to since I didn't want to have too many and it might have become confusing. It related that you would get the best medical care of your lifetime – after you died, when they were rushing to save your organs, for transplant. Obviously this would not be true if you were not an organ donor (at least in this country) or died as the result of general wasting away so that you had nothing left which would be particularly coveted. But this is a major issue in medicine in some countries and there have been various lurid tales of bodies being robbed of their organs without family permission, bodies of Ukrainian soldiers harvested of their organs and rackets in third-world countries where the poor or helpless are robbed of organs while they are alive. From my standpoint, since I haven't done much research on it, I have seen little proof of any of them despite plenty of allegation, but it is easy to understand that traffic in organs to those who will pay anything to live a little longer would be tremendously profitable, and the potential for disproportionate profit seldom fails to draw the unscrupulous.Patient Observer , November 28, 2017 at 12:49 pmAs I alluded in the lead-in, Canada has what is sometimes described as 'socialized medicine' and alternatively as 'two-tier healthcare' although I have never seen any real substantiation for the latter charge. My mom had an operation for colon cancer some time back, and she paid nothing for the hospitalization or the operation. My father-in-law is scheduled for the same operation as soon as he gets his blood-sugar low enough, and he already had one for a hernia and removal of internal scar tissue from an old injury – again, we paid nothing. He had a nurse come here for a couple of months, once a week, to change his dressing (because the incision would was very slow to heal because he is diabetic – nothing. That's all great, from my point of view, and I've paid into it all my life without ever using it because I was covered by the government under federal guidelines while I served in the military, although I was a cheap patient because I never had to be hospitalized for anything and was almost never even sick enough not to come to work. But the great drawback to it, as I said, is the backlog which might mean you have to wait too long for an operation. And in my small practical experience – the two cases I have just mentioned – both were scheduled for surgery within a month of diagnosis. So perhaps the long wait is for particular operations such as heart or brain surgery.
The Albanian Kosovo Liberation Army harvested organs from captured Serb civilians and soldiers:et Al , November 28, 2017 at 1:32 amhttps://thebloodyellowhouse.wordpress.com/
In December 14th 2010, Dick Marty, Rapporteur of EU Commission pass for adoption to the Council of Europe a report on allegations of inhuman treatment of people and illicit trafficking in human organs in Kosovo organized by KLA leader and Kosovo Prime minister Hashim Thaçi . An official report accusing Kosovo's prime minister of links to a "mafia-like" network that killed captives in order to sell their organs on the black market was yesterday endorsed by a Council of Europe committee.
Bold text emphasis added.
Nothing came of the charges that I am aware of and it is business as usual with Kosovo and Albania.
Per Wikipedia:
The Washington Times reported that the KLA was financing its activities by trafficking the illegal drugs of heroin and cocaine into western Europe.[16]
A report to the Council of Europe, written by Dick Marty, issued on 15 December 2010[23] states that Hacim Thaçi was the leader of the "Drenica Group" in charge of trafficking organs taken from Serbian prisoners.
On 17 February 2008, Kosovo declared its independence from Serbia. Thaçi became Prime Minister of the newly independent state.
So, there you have it – the war criminal, drug runner, murderer and organ thief/butcher became the PM of Kosovo, a nation created and nurtured by NATO with a nod and a wink from the EU. Simply disgusting but typical treatment for Serbia by the fascist/racist and genocidally inclined West.
Thank you very much for a very interesting article UCG! Quite the horror story. I've heard quite a few about the US over the years from people I know too. I think one of the BBC's former America correspondent gave an interview to the Beeb as he was leaving America a few years back (MAtt Frei?) and was asked what were the best and worst things about living there. The worst was certainly healthcare.yalensis , November 28, 2017 at 3:21 amI've also read that healthcare costs for the self-employed, independents, freelancers can also be crushing in the land of the free where everyone can become rich. Has this changed? I would have thought that those were the ideal Americans, making it off their own back, but apparently not.
There's also another issue that is not addressed: an ageing population. This is a very current theme and it is now not at all unusual for people to live another 30 odd years after retirement. Now how on earth will such people manage their healthcare for such a period? Will they have to hock absolutely everything they have? America is already at war with itself (hence the utmost need to for foreign enemies), but nothing is getting done. Just more of the same. Meanwhile the Brits are trying to copy the US through stealth privatization of their health system. It might work as well as privatizing its rail service
Thanks for an interesting post, UCG. Hopefully this will stimulate some ideas on how to fix the American healthcare system, which seems to be badly broken.Patient Observer , November 28, 2017 at 4:34 amBroken for us but working perfectly for Big Pharma and insurance companies. That is a fundamental reason why it will be extremely difficult to "fix" because it ain't broken as a money making machine.yalensis , November 28, 2017 at 1:25 pmTrue. And the insurance companies, in particular, have been really raking it in, especially with Obamacare and the various Medicare Advantage options.Ryan Ward , November 28, 2017 at 3:40 amWith health care in general, there's a bit of a trade-off. The most cost-efficient systems, like the system in Sweden for example, are fairly regimented and don't leave much room for individual choice (unless someone pays out of pocket for treatment completely outside the public system). On the other hand, systems that give people a little more choice, like the system in Germany, tend to be a little on the pricey side. I think, given American political culture, something along the lines of the German model is much more likely to attract widespread public support. In any case, it's still cheaper than the American system, and achieves some of the best results in the world. https://en.wikipedia.org/wiki/Healthcare_in_Germany
Nov 15, 2017 | www.nakedcapitalism.com
Alex Azar: Can There Be Uglier Scenarios than the Revolving Door? Posted on November 15, 2017 by Lambert Strether By Lambert Strether
Clearly, Alex Azar, nominated yesterday for the position of Secretary of Health and Human Services by the Trump Administration, exemplifies the case of the "revolving door," through which Flexians slither on their way to (or from) positions of public trust. Roy Poses ( cross-posted at NC ) wrote, when Azar was only Acting Secretary:
Last week we noted that Mr Trump famously promised to “drain the swamp” in Washington. Last week, despite his previous pledges to not appoint lobbyists to powerful positions, he appointed a lobbyist to be acting DHHS Secretary. This week he is apparently strongly considering Mr Alex Azar, a pharmaceutical executive to be permanent DHHS Secretary, even though the FDA, part of DHHS, has direct regulatory authority over the pharmaceutical industry, and many other DHHS policies strongly affect the pharmaceutical industry. (By the way, Mr Azar was also in charge of one lobbying effort.)
So should Mr Azar be confirmed as Secretary of DHHS, the fox guarding the hen house appears to be a reasonable analogy.
Moreover, several serious legal cases involving bad behavior by his company, and multiple other instances of apparently unethical behavior occurred on Mr Azar’s watch at Eli Lilly. So the fox might be not the most reputable member of the species.
So you know the drill…. The revolving door is a species of conflict of interest . Worse, some experts have suggested that the revolving door is in fact corruption. As we noted here , the experts from the distinguished European anti-corruption group U4 wrote ,
The literature makes clear that the revolving door process is a source of valuable political connections for private firms. But it generates corruption risks and has strong distortionary effects on the economy , especially when this power is concentrated within a few firms.
The ongoing parade of people transiting the revolving door from industry to the Trump administration once again suggests how the revolving door may enable certain of those with private vested interests to have excess influence, way beyond that of ordinary citizens, on how the government works, and that the country is still increasingly being run by a cozy group of insiders with ties to both government and industry. This has been termed crony capitalism.
Poses is, of course, correct. (Personally, I've contained my aghastitude on Azar, because I remember quite well how Liz Fowler transitioned from Wellpoint to being Max Baucus's chief of staff when ObamaCare was being drafted to a job in Big Pharma , and I remember quite well the deal with Big Pharma Obama cut, which eliminated the public option , not that the public option was anything other than a decreasingly gaudy "progressive" bauble in the first place.)
In this post, I'd like to add two additional factors to our consideration of Azar. The first: Democrat credentialism makes it hard for them to oppose Azar. The second: The real damage Azar could do is on the regulatory side.[1]
First, Democrat credentialism. Here is one effusive encomium on Azar. From USA Today, "Who is Alex Azar? Former drugmaker CEO and HHS official nominated to head agency" :
"I am glad to hear that you have worked hard, and brought fair-minded legal analysis to the department," Democratic Sen. Max Baucus said at Azar's last confirmation hearing.
And:
Andy Slavitt, who ran the Affordable Care Act and the Centers for Medicare & Medicaid Services during the Obama administration, said he has reason to hope Azar would be a good secretary.
"He is familiar with the high quality of the HHS staff, has real-world experience enough to be pragmatic, and will hopefully avoid repeating the mistakes of his predecessor," Slavitt said.
So, if Democrats are saying Azar is "fair-minded" and "pragmatic" -- and heaven forfend that the word "corruption"[2] even be mentioned -- how do they oppose him, even he's viscerally opposed to everything Democrats supposedly stand for? (Democrats do this with judicial nominations, too.) Azar may be a fox, alright, but the chickens he's supposedly guarding are all clucking about how impeccable his qualifications are!
Second, let's briefly look at Azar's bio. Let me excerpt salient detail from USA Today :
1. Azar clerked for Supreme Court Justice Antonin Scalia .
2. Azar went to work for his mentor, Ken Starr , who was heading the independent counsel investigation into Bill and Hillary Clinton's Whitewater land deal.
3. Azar had a significant role in another major political controversy when the outcome of the 2000 presidential election hinged on a recount in Florida . Azar was on the Bush team of lawyers whose side ultimately prevailed [3]
For any Democrat with a memory, that bio provokes one of those "You shall know them by the trail of the dead" moments. And then there's this:
When Leavitt replaced Thompson in 2005 and Azar became his deputy, Leavitt delegated a lot of the rule-making process to Azar.
So, a liberal Democrat might classify Azar as a smooth-talking reactionary thug with a terrible record and the most vile mentors imaginable, and on top of it all, he's an effective bureaucratic fixer. What could the Trump Administration possibly see in such a person? Former (Republican) HHS Secretary Mike Leavitt explains:
"Understanding the administrative rule process in the circumstance we're in today could be extraordinarily important because a lot of the change in the health care system, given the fact that they've not succeeded legislatively, could come administratively."
We outlined the administration strategy on health care in "Trump Adminstration Doubles Down on Efforts to Crapify the Entire Health Care System (Unless You're Rich, of Course)" . There are three prongs:
1) Administratively, send ObamaCare into a death spiral by sabotaging it
2) Legislatively, gut Medicaid as part of the "tax refom" package in Congress
3) Through executive order, eliminate "essential health benefits" through "association health plans"
As a sidebar, it's interesting to see that although this do-list is strategically and ideologically coherent -- basically, your ability to access health care will be directly dependent on your ability to pay -- it's institutionally incoherent, a bizarre contraption screwed together out of legislation, regulations, and an Executive order. Of course, this incoherence mirrors to Rube Goldberg structure of ObamaCare itself, itself a bizarre contraption, especially when compared to the simple, rugged, and proven single payer system. ( Everything Obama did with regulations and executive orders, Trump can undo, with new regulations and new executive orders . We might compare ObamaCare to a child born with no immune system, that could only have survived within the liberal bubble within which it was created; in the real world, it's not surprising that it's succumbing to opportunistic infections.[2])
On #1, The administration has, despite its best efforts, not achieved a controlled flight into terrain with ObamaCare; enrollment is up. On #2, the administration and its Congressional allies are still dickering with tax reform. And on #3 . That looks looks like a job for Alex Azar, since both essential health benefits and association health plans are significantly affected by regulation.
So, yes, there are worse scenarios than the revolving door; it's what you leave behind you as the door revolves that matters. It would be lovely if there were a good old-fashioned confirmation battle over Azar, but, as I've pointed out, the Democrats have tied their own hands. Ideally, the Democrats would junk the Rube Goldberg device that is ObamaCare, rendering all of Azar's regulatory expertise null and void, but that doesn't seem likely, given that they seem to be doing everything possible to avoid serious discussion of policy in 2018 and 2020.
NOTES
[1] I'm leaving aside what will no doubt be the 2018 or even 2020 issue of drug prices, since for me that's subsumed under the issue of single payer. If we look only at Azar's history in business, real price decreases seem unlikely. Business Insider :
Over the 10-year period when Azar was at Lilly, the price of insulin notched a three-fold increase. It wasn't just Lilly's insulin product, called Humalog. The price of a rival made by Novo Nordisk has also climbed, with the two rising in such lockstep that you can barely see both trend lines below.
The gains came despite the fact that the insulin, which as a medication has an almost-century-long history, hasn't really changed since it was first approved.
Nice business to be in, eh? Here's that chart:
It's almost like Lilly (Azar's firm) and Novo Nordisk are working together, isn't it?
[2] Anyhow, as of the 2016 Clinton campaign , the Democrat standard -- not that of Poses, nor mine -- is that if there's no quid pro quo, there's no corruption.
[3] And, curiously, "[HHS head Tommy] Thompson said HHS was in the eye of the storm after the 2001 terrorist attacks, and Azar had an important role in responding to the resulting public health challenges, as well as the subsequent anthrax attacks "
MedicalQuack , November 15, 2017 at 10:31 am
diptherio , November 15, 2017 at 11:25 amOh please, stop quoting Andy Slavitt, the United Healthcare Ingenix algo man. That guy is the biggest crook that made his money early on with RX discounts with his company that he and Senator Warren's daughter, Amelia sold to United Healthcare. He's out there trying to do his own reputation restore routine. Go back to 2009 and read about the short paying of MDs by Ingenix, which is now Optum Insights, he was the CEO and remember it was just around 3 years ago or so he sat there quarterly with United CEO Hemsley at those quarterly meetings. Look him up, wants 40k to speak and he puts the perception out there he does this for free, not so.
a different chris , November 15, 2017 at 2:01 pmI think you're missing the context. Lambert is quoting him by way of showing that the sleazy establishment types are just fine with him. Thanks for the extra background on that particular swamp-dweller, though.
petal , November 15, 2017 at 12:52 pmNot just the context, it's a quote in a quote. Does make me think Slavitt must be a real piece of work to send MQ so far off his rails
sgt_doom , November 15, 2017 at 1:21 pmAlex Azar is a Dartmouth grad (Gov't & Economics '88) just like Jeff Immelt (Applied Math & Economics '78). So much damage to society from such a small department!
Jen , November 15, 2017 at 7:56 pmNice one, petal !!!
Really, all I need to know about the Trumpster Administration:
From Rothschild to . . . .
https://en.wikipedia.org/wiki/Wilbur_Ross
Since 2014, Ross has been the vice-chairman of the board of Bank of Cyprus PCL, the largest bank in Cyprus.
He served under U.S. President Bill Clinton on the board of the U.S.-Russia Investment Fund. Later, under New York City Mayor Rudy Giuliani, Ross served as the Mayor's privatization advisor.
jo6pac , November 15, 2017 at 2:13 pmOr from a "small liberal arts college" (which is a university in all but name, because alumni).
Tim Geitner ('82 – Goverment)
Hank Paulson ('68 – English)Alfred , November 15, 2017 at 2:53 pmWell it's never ending game in the beltway and we serfs aren't in it.
https://consortiumnews.com/2017/11/15/trump-adds-to-washingtons-swamp/
I don't believe that the President's "swamp" ever consisted of crooked officials, lobbyists, and cronies I think it has always consisted of those regulators who tried sincerely to defend public interests.
It was in the sticky work of those good bureaucrats that the projects of capitalists and speculators bogged down. It is against their efforts that the pickup-driving cohort of Trump_vs_deep_state (with their Gadsden flag decals) relentlessly rails.
Trump has made much progress in draining the regulatory swamp (if indeed that is the right way to identify it), and no doubt will make considerably more as time wears on, leaving America high and dry. The kind of prevaricator Trump is may simply be the one who fails to define his terms.
Henry Moon Pie , November 15, 2017 at 4:13 pm
I think we've moved past the revolving door. We hear members of the United States Senate publicly voice their concerns about what will happen if they fail to do their employers' bidding (and I'm not talking about "the public" here). In the bureaucracy, political appointees keep accruing more and more power even as they make it clearer and clearer that they work for "the donors" and not the people. Nowhere is this more true than the locus through which passes most of the money: the Pentagon. The fact that these beribboned heroes are, in fact, setting war policy on their own makes the knowledge that they serve Raytheon and Exxon rather than Americans very, very troubling.
I suspect Azar's perception is that he is just moving from one post to another within the same company.
Watt4Bob , November 15, 2017 at 5:28 pm
Larry , November 15, 2017 at 8:01 pmPerfect cartoon over at Truthout
I'm amazed there is enough private security available on this planet to keep these guys safe.
Big pharma indeed has so much defense from the supposed left. It combines their faith in technological progress, elite institutions, and tugs on the heart strings with technology that can save people from a fate of ill health or premature death. Of course, the aspect of the laws being written to line the pockets of corrupt executives is glossed over. While drug prices and medical costs spiral ever higher, our overall longevity and national health in the US declines. That speaks volumes about what Democrats really care about.